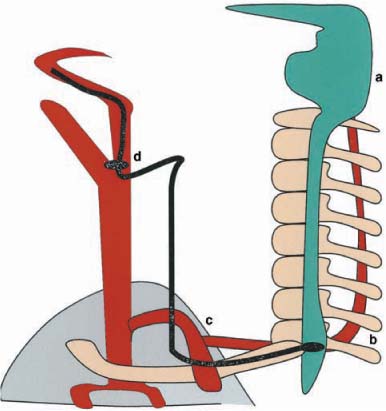
Chapter 36 Horner’s syndrome is caused by dysfunction of the sympathetic innervation to the eye and to parts of the face. Initial evaluation is aimed at confirming loss of sympathetic innervation, characterizing the anatomic level of loss (i.e., postganglionic versus preganglionic) and referring the patient for ancillary testing to uncover the cause. A patient with suspected new Horner’s syndrome, if experiencing pain, should be evaluated the same day to determine if the history or accompanying signs and symptoms suggests complication-prone disorders such as dissection of the internal carotid artery. Patients without pain may be evaluated within a week. The first-order sympathetic neuron begins in the ipsilateral hypothalamus, and descends through the midbrain, pons, and medulla to end at the ciliospinal center of Budge, in the spinal cord, at levels C8-T1 (Fig. 36–1). Preganglionic second-order sympathetic fibers leave the ciliospinal center of Budge, pass the pulmonary apex, traveling up along the carotid artery sheath, and ending in the superior cervical ganglion near the bifurcation of the common carotid artery. From the superior cervical ganglion, the third-order postganglionic neuron travels along the internal carotid artery (ICA) and into the cavernous sinus. In the cavernous sinus, sympathetic postganglionic fibers leave the ICA, travel with the abducens nerve for a brief course, join the ophthalmic division of the trigeminal nerve, and enter the orbit with the nasociliary branch. The sympathetic fibers pass through the ciliary ganglion without synapsing and join the two long ciliary branches of the nasociliary nerve, reaching the anterior segment of the eye and inner-vating the iris dilator muscle. Other sympathetic branches travel with branches of the ophthalmic artery to innervate the lacrimal gland, Müller’s muscles and the orbital vessels. Sympathetic fibers controlling sweating of the face travel with the external carotid artery (ECA). One to 2 mm of upper eyelid ptosis occurs due to paralysis of the sympathetically innervated Müller muscles, a smooth muscle that contributes to the position of the upper eyelid (Fig. 36–2). Slight elevation of the lower eyelid is a result of loss of the sympathetic innervation to the smooth muscle fibers of the lower eyelid (Fig. 36–2). The dilator muscle of the iris is sympathetically innervated. In Horner’s syndrome the pupil is constricted (Fig. 36–2). Anisocoria in Horner’s syndrome is greater in darkness, when the dilator muscle of the iris is normally more active. The degree of anisocoria may also increase when the patient is alert or excited (increased sympathetic tone resulting in greater dilation of the normal pupil), and may decrease when the patient is drowsy. FIGURE 36–1 Diagram depicting sympathetic anatomy of the eye and face. a, midbrain; b, cilio-spinal center; c, pulmonary apex; d, superior cervical ganglion. Prolonged redilation of the pupil after dimming the light is more diagnostic than comparing pupil diameter.1 Adding a sudden loud noise at the time of light dimming further increases the anisocoria by further stimulation of the sympathetically driven dilation of the unaffected pupil. FIGURE 36–2 An 11-year-old boy with congenital Horner’s syndrome from suspected perinatal injury. Note typical features of Horner’s syndrome in the right eye, including upper lid ptosis, reversed ptosis of the lower lid (less sclera is visible on the right compared with the left eye), miosis of the pupil on the affected side, and hypochromia iridis. Hypochromia iridis is a feature typical of congenital Horner’s syndrome, but may occur in acquired forms as well.2 Central (first-order) Horner’s syndrome is often accompanied by anhidrosis of the entire ipsilateral half of the body. Preganglionic (second-order) Horner’s is usually associated with loss of sweating and flushing on the affected side of face and neck, though usually unnoticed by the patient. Cocaine blocks the reuptake of norepinephrine into the sympathetic nerve endings, making this neuro-transmitter more available at the motor end plate. In a normal eye, two drops of a 10% cocaine solution cause dilation of the pupil, maximally noticed after 45 to 60 minutes in dim lighting. Patient should be active (e.g., walking) while waiting for the cocaine test. In a sympathetically denervated pupil no dilation occurs. Although traditionally one looks for at least a 1-mm increase in anisocoria from the drops, in skilled hands it is unnecessary to compare the anisocoria before and after cocaine instillation, because a postcocaine anisocoria of 0.8 mm is sufficient to diagnose a Horner’s syndrome3 (Figs. 36–3 and 36–4). Patients undergoing pharmacological testing for Horner’s syndrome should be warned that substance abuse testing of their urine may remain positive for several days.4 Postganglionic (third-order) Horner’s syndrome is differentiated from preganglionic (first- or second-order) Horner’s syndrome by the hydroxyamphetamine test.5 This test should be performed at least 48 hours after cocaine instillation to ensure maximal sensitivity.6 Hydroxyamphetamine releases norepinephrine from stores in the nerve endings, resulting in mydriasis in a normal pupil. After ~2 weeks of postganglionic denervation the nerve endings are destroyed, so that no mydriasis is produced in response to hydroxyamphetamine instillation. After this period of denervation, a postganglionic Horner’s pupil develops denervation supersensitivity and dilates more than its fellow normal pupil in response to a weak adrenergic drop such as 1% phenylephrine; 1% Polhedrine solution, the n-methyl derivative of hydroxyamphetamine, may be substituted for 0.5% hydroxyamphetamine if it is easier to obtain.7 FIGURE 36–3 Pharmacological testing with 10% cocaine eye drops. Note typical features of Horner’s syndrome before testing. Central (first-order) Horner’s syndrome is diagnosed by the “company it keeps” (accompanying signs and symptoms; see later) and by pharmacological testing indicating a preganglionic Horner’s syndrome. After distinguishing between a postganglionic and preganglionic Horner’s syndrome, a careful history and physical examination often helps to focus the diagnostic ancillary testing.
HORNER’S SYNDROME
URGENCY OF EVALUATION
SYMPATHETIC ANATOMY OF THE EYE AND FACE
DIAGNOSIS
SIGNS
Ptosis
Reverse-Ptosis
Miosis
Anisocoria
Dilation Lag

Hypochromia Iridis
Anhidrosis
PUPIL TESTING (SEE CHAPTER 2)
PHARMACOLOGICAL CONFIRMATION OF HORNER’S SYNDROME
LOCALIZATION

DIFFERENTIAL DIAGNOSIS
CENTRAL HORNER’S SYNDROMES
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


