Pediatric Ophthalmology
Edited by P. F. Gallin
Thieme Medical Publishers, Inc.
New York ©2000

14

Horizontal Strabismus Surgery
This chapter is written with the assumption that the patient is in need of surgery on the horizontal rectus muscles to treat esotropia or exotropia. The selection of surgery for treating the esotropia may be recession of the medial rectus muscles of each eye, or only one eye, or possibly a recession of the medial rectus and resection of the lateral rectus muscles of the same eye. For exotropia the recession may be of the lateral rectus in either one or both eyes, or it could be a recession of the lateral rectus combined with a resection of the medial rectus on the same eye. These procedures, the most common and straightforward extraocular muscle surgery procedures, will be illustrated in this chapter.1
 Preoperative Preparation
Preoperative Preparation
The patient is positioned at the end of the operating table. The patient’s chin is elevated throughout the surgery, which is accomplished best by having a shoulder roll under the patient’s upper chest and shoulder. This assures that the neck will be extended, keeping the face in a 20- to 30-degree chin-up position, which makes it easier for the sitting surgeon and assistant to do the surgery. If the surgeon and assistant stand, it probably is not important to place the head in a chin-up position. However, most ophthalmic surgeons sit because this position offers better control for fine hand movements because it allows them to anchor their elbows against their rib cage.
The face is prepped with Betadine solution, and a half concentration of Betadine is irrigated into the eyes followed by an irrigation of sterile saline solution. The patient is draped, the eyelid speculum is placed, and surgery is ready to begin.
 The Incision
The Incision
Access to the extraocular muscles is through the 10-mm area that extends between the limbus and conjunctival cul de sac behind the eyelids. The eye speculum exposes this access zone very well. All four rectus muscles insert within the surgical access zone. The first objective of the surgeon is to make an incision through the conjunctiva, Tenons, and intermuscular septum down to the sclera so that a muscle hook can be introduced under the muscle to engage the tendon at its insertion.
The surgeon has only two options in choosing the site for making the incision. The incision should be either limbal or in the fornix. Never place the incision over the surface of the rectus muscle because incised tissue heals by scarring to its surrounds. An incision made over the surface of the rectus muscle results in adherence of the overlying Tenons and conjunctiva to the underlying capsule of the rectus muscle. With time, the scar cicatrizes, pulling the eye out of the desired alignment and restricting the full duction amplitude that the muscle is capable of delivering. Moreover, if secondary surgery is required, the separation of the scarred conjunctiva, Tenons, and muscle capsule requires sharp dissection, which is bloody because the muscle bleeds profusely as soon as its capsule is nicked. After the secondary surgery the same undesirable scarring of the muscle to the same surrounding tissues will recur, and the process is destined to repeat itself. To avoid this chain of events, the incision must be placed away from the rectus muscle at the initial surgery. By placing the incision at the limbus or in the fornix between neighboring rectus muscles, the undesirable scarring process is avoided.
The advantage of the limbal incision (Figs. 14-1 through 14-3) is that it offers a direct route to the muscle. Its main disadvantage is the discomfort the patient experiences from the incision adjacent to the copious corneal nerves.
Other disadvantages include the formation of a circumlimbal mound of tissue, from the edematous conjunctiva adjacent to the cornea, that can interfere with covering of the neighboring corneal epithelium by the tear film, resulting in a dellen, and a visible incisional scar.
The advantages of the fornix incision (Figs. 14-4 through 14-6) are that it is hidden behind the lower eyelid, the patient is comfortable, and the potential complication of a dellen is eliminated. The disadvantage is that the surgeon must first slide the conjunctiva and Tenons over the rectus muscle before it is visualized, and these layers of tissue must be retracted while suturing the muscle onto the sclera. For the inexperienced strabismus surgeon, anatomic landmarks are often “misplaced” while recessing the muscle.
The two incisions are illustrated in Figures 14-1 through 14-6. To demonstrate the incisions, surgery on the right medial rectus muscle has been chosen. The eye speculum is a Lancaster (Storz E-4056). For a small child a better speculum is the Barraquer child size (Storz E-4107). While the assistant positions the eye with Lester fixation forceps (Storz E-1656), either incision is made with the Westcott tenotomy scissors (Storz E-3321).
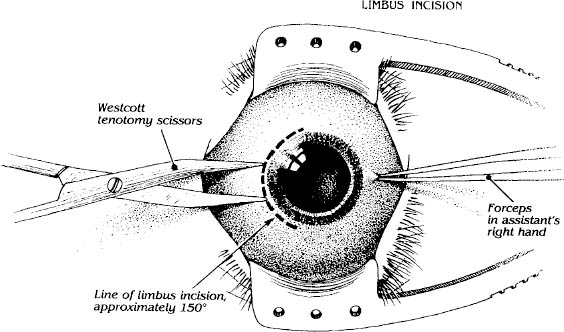
FIGURE 14-1. The limbal incision. The assistant positions the eye in 10-degree abduction with a Lester fixation forceps. (Parks MM. Atlas of Strabismus Surgery. Philadelphia: Harper & Row; 1983:79.)
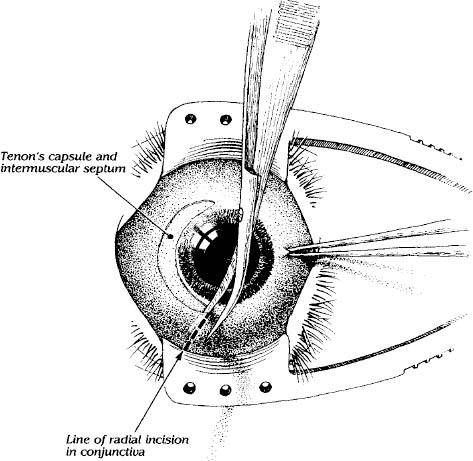
FIGURE 14-2. The conjunctival incision is enlarged by an 8-mm radial cut from the superior end of the limbal portion of the conjunctival incision. (Parks MM. Atlas of Strabismus Surgery. Philadelphia: Harper & Row; 1983:82.)
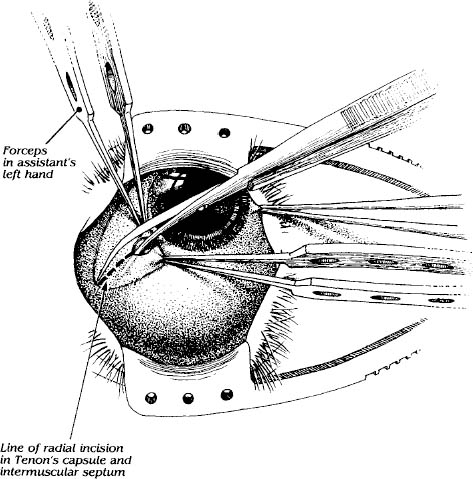
FIGURE 14-3. The radial cut is through Tenons and intermuscular septum, which exposes the sclera between the medial and superior rectus muscles. The eye is displaced interiorly by the assistant while both the assistant and surgeon elevate Tenons and intermuscular septum with Bishop-Harmon forceps (Parks MM. Atlas of Strabismus Surgery. Philadelphia: Harper & Row; 1983:83.) This may be repeated routinely in the inferior medial quadrant by the same surgeons.
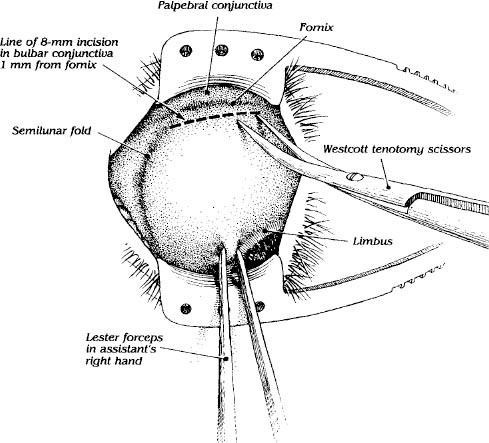
FIGURE 14-4. The fornix incision is not literally in the fornix; it is 2 mm above the fornix in the bulbar conjunctiva. It is 8 mm long with the nasal terminus for the inferomedial incision at the semilunar fold (plica). The tips of the open scissors are gently pushed perpendicularly into the conjunctiva, closed, which incises the conjunctiva for 3 mm. This maneuver is repeated in approximately three steps completing the conjunctival incision. (Parks MM. Atlas of Strabismus Surgery. Philadelphia: Harper & Row; 1983:71.)
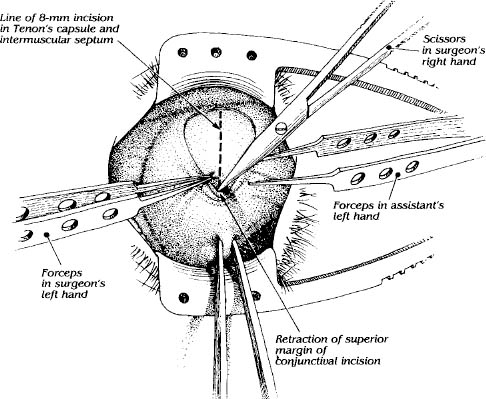
FIGURE 14-5. While the eye is held upward and abducted by the assistant, the surgeon using the closed scissors retracts upward the superior margin of the conjunctival incision. Both the assistant and the surgeon with their free hand grasp and raise the combined Tenons and intermuscular septum with forceps, which is incised by the surgeon, revealing the sclera. (Parks MM. Atlas of Strabismus Surgery. Philadelphia: Harper & Row; 1983:74.)
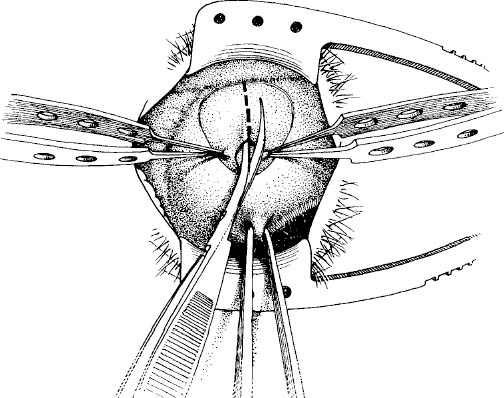
FIGURE 14-6. The incision of Tenons and intermuscular septum is completed. The incision should never go beyond the fornix; otherwise, bleeding will be profuse as the very vascular extraconal fat is incised. (Parks MM. Atlas of Strabismus Surgery. Philadelphia: Harper & Row; 1983:76.)
 The Dissection of the Muscle
The Dissection of the Muscle
Having completed the incisions and being able to visualize the sclera, the surgeon now turns to dissecting the horizontal rectus muscle. A Stevens tenotomy hook (Storz E-600) is slipped under the insertion of the right medial muscle in a manner that does not traumatize it (Fig. 14-7
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


