Chapter 1 History of Thyroid and Parathyroid Surgery
The history of thyroid surgery documents the evolution of modern surgical techniques and the blending of these techniques with an expanded understanding of anatomy and endocrinology. The road has had many twists. Even when thyroid and parathyroid disorders were first recognized as discrete entities, they were misunderstood. Initially, Graves’ disease was felt to represent a cardiac illness, hypothyroidism a neurologic and dermatologic disorder, and hyperparathyroidism a primary bone disorder. One of the first thyroid procedures in the 1600s resulted in the imprisonment of the surgeon.2 Fortunately, the anatomist and physiologist embraced the initial morbid surgical misadventures, ultimately rendering the applied art of thyroid surgery a safe and even triumphant treatment form. As Halsted has written, “The extirpation of the thyroid gland for goiter typifies perhaps better than any other operation the supreme triumph of the surgeon’s art.”3 The surgical story begins with the treatment of iodine deficiency.
The Early Years
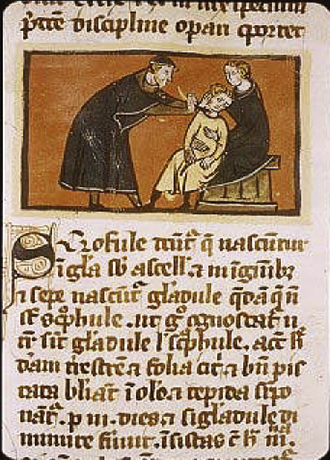
Early developments in thyroid surgery came from the school of Salerno, Italy, in the 12th and 13th centuries (Figure 1-1). The typical operation involved insertion of two heated iron setons at right angles into the offending mass. These were then manipulated at the skin surface twice a day until they pierced the flesh. In cases in which arterial supply of the goiter was thought not to be excessive, the surface of the goiter was cut, the tumorous tissue was grasped with a hook, and the skin was dissected away from it. Once exposed, the section of goiter with its capsule would be removed with a finger. Pedunculated goiters would be ligated en masse with a bootlace and removed.4 During such procedures, patients were tied down to a table and held firmly. Although these procedures sometimes reduced goiter size, patients often died from sepsis or hemorrhage.4
The anatomy of the normal thyroid gland was not generally understood until the Renaissance, through the work of Leonardo da Vinci (Figure 1-2). He drew the thyroid as two globular glands, which he speculated filled up empty spaces in the neck (Figure 1-3).5 Others pondered the function of the thyroid gland, speculating that its role was to lubricate the neck or make it more aesthetically pleasing. Caleb Hillier Parry of Bath, England, recognizing the thyroid gland’s vascularity, considered the gland a blood buffer to protect the brain from sudden increases in blood flow from the heart.6 In Roman times, increased neck girth was believed to herald the onset of puberty.7 Bartholomeo Eustachius of Rome in the 16th century characterized the gland as “glandulam thyroideam” with two lobes connected via an isthmus.4 The term thyroid gland (glandula thyroideois) is attributed to Thomas Wharton (described in his work Adenographia) (1646); he gave this name because of either the gland’s own shieldlike shape (thyreos: Greek “shield”) or because of the shape of the thyroid cartilage, with which it is closely associated.8

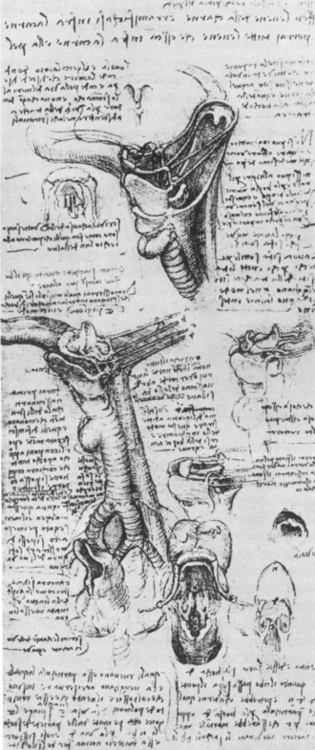
Figure 1-3 The first illustration of a thyroid is attributed to Leonardo da Vinci in 1503.
(From O’Malley CD, de CM Saunders JB: Leonardo on the human body, New York, 1983, Dover Publications, p. 169.)
In 1646, Wilhelm Fabricus reported the first thyroidectomy performed using scalpels. However, the patient, a 10-year-old girl, died and the surgeon was imprisoned.2 In 1791, Pierre Joseph Desault performed a successful partial thyroidectomy in Paris.2 Guillaume Dupuytren followed in Desault’s footsteps and in 1808 performed the first “total” thyroidectomy. Unfortunately, despite little intraoperative blood loss, the patient died of “shock.”2 The most successful thyroid surgeon of that time was Johann Hedenus, a German surgeon from Dresden. By 1821 he had reported on the successful removal of six large obstructing goiters. His remarkable series would not be equaled for nearly 40 years.5 In the 1850s, a variety of incisions—longitudinal, oblique, and, occasionally, Y-shaped—were performed for thyroidectomy. Collar incision had been introduced by Jules Boeckel of Strasbourg in 1880.2 After skin incisions, most surgeons at this time performed blunt dissection. Bleeding was generally inadequately controlled. Bloodletting was performed for postoperative complications, despite perioperative blood loss. Typically, wounds were left open, and dead spaces were either packed or left to fill with blood.4
The progress of early thyroid surgery is intertwined with initial advances in our understanding of thyroid endocrinology. It had been known empirically for some time that seaweed kelp and marsh seawater reduced goiter size. In 1811, Bernard Courtois discovered iodine in burned seaweed.5 By 1820, Johann Straub and Francois Coindet, both Swiss, systematically studied the use of iodine to treat goiter. Coindet went on to recommend the use of iodine preoperatively to reduce the size and vascularity of goiters and, therefore, lessen operative risks.4 The use of iodine preparations became widespread. Considered miracle drugs, iodine medications were abused, and toxicity often resulted.9 In the 1830s, Robert Graves’ and Karl von Basedow initially described toxic diffuse goiter through recognition of the “Merseburg triad” of goiter, exophthalmos, and palpitations.10,11 Interestingly, despite being attributed to Graves’ and Basedow, the association of goiter and orbital disease was described already in the 11th century by two Persian physicians, Avicenna and Aj-Jurjani.12
Can the thyroid gland, when in a state of enlargement, be removed with a reasonable hope of saving the patient? Experience emphatically answers NO.… If a surgeon should be so foolhardy as to undertake it … every step of the way will be environed with difficulty, every stroke of his knife will be followed by a torrent of blood, and lucky will it be for him if his victim lives long enough to enable him to finish his horrid butchery. No honest and sensible surgeon would ever engage in it!13
The Surgical Revolution
The surgical revolution began with the pivotal discovery of anesthesia, as it was subsequently termed by Oliver Wendell Holmes.14 In 1842, Crawford W. Long, from Georgia, was the first to use sulfuric ether as an anesthetic during surgery.9 The era of modern surgical anesthesia truly began with William Morton’s demonstration of ether’s efficacy at Massachusetts General Hospital in Boston in 1846.9 In 1847, in Vladikavkaz, Russia, Nikolai Pirogov was the first surgeon to use general anesthesia during a thyroidectomy.2 The patient was a 17-year-old girl with a goiter causing compression of the trachea.15 The surgery was quite difficult since the “tumor was of a size of an apple” and “more than 30 ligatures were required.” The wound healing was complicated “with pus.” The outcome of surgery was nevertheless a success. Soon Pirogov performed three more thyroid surgeries in St. Petersburg. He never placed sutures on the wound edges fearing erysipelas and “purulent pockets.”16
The introduction of antisepsis by Joseph Lister in 1867 was the second step in the surgical revolution. Lister’s concept was quickly adopted in continental Europe but was met with some resistance in Great Britain and the United States.5 Theodor Kocher and Albert Theodor Billroth, fathers of modern thyroid surgery, adopted Lister’s antisepsis concepts in the 1870s. Gustav Neuber introduced the concept of intraoperative asepsis in 1883 when he brought the cap and gown into the operating theater. In 1886, Ernst von Bergmann of Berlin introduced steam sterilization of surgical instruments.17
The final step in the development of modern surgery was improved hemostasis, made possible because of new surgical instrumentation introduced by Spencer Wells. He devised a simple, self-retaining arterial forceps (with one catch) in 1872 and reported on its use in 1874.18 Additional improvements of the forceps, such as reduction in its weight and inclusion of more ratcheted catches, transformed surgical technique by reducing operative bleeding and, ultimately, mortality.
With patients’ pain and motion better controlled by anesthesia and hemostasis improved by better hemostatic forceps, surgeons had more time to attend to the underlying anatomy, allowing for more successful thyroidectomy with a safe, nonseptic postoperative course. Consequently, from 1850 to 1875, mortality from thyroid surgery was reduced by half.2
Development of Modern Thyroid Surgery
Albert Theodor Billroth (1829-1894) is generally regarded as the most distinguished surgeon of the 19th century. He was born the son of a German clergyman in 1829 (Figure 1-4). Appointed at the age of 31 to the chair at Zurich, he cautiously undertook the surgical treatment of obstructive goiters endemic to this area. During his first 6 years in Zurich, he performed 20 thyroidectomies. He courageously published the results, noting a mortality rate of approximately 40%. Mortality was primarily due to postoperative sepsis and intraoperative hemorrhage. Billroth considered this mortality rate disastrous, and he virtually abandoned the procedure for almost a decade.13 He regained confidence in performing thyroid surgery in 1877, after the advent of antisepsis (which he was initially slow to embrace) and improved instrumentation. At that time, the mortality rate from his procedure fell to 8%. Billroth’s procedure typically involved division of the sternocleidomastoid muscle and incision and drainage of any thyroid cysts. Hemostasis was achieved through arterial ligation and the use of aneurysmal needles and an Indian vegetable styptic, punghawar djambi.

Figure 1-4 Albert Theodor Billroth, 1867.
(Reproduced with permission from Institut für Medizingeschichte, Universität Bern, Buehlstrasse 26, CH 3012 Bern.)
Theodor Kocher (1841-1917)
It is, however, Theodor Kocher who stands alone in the annals of thyroid surgery. The work of Kocher (Figure 1-5) was instrumental in the development of modern thyroidectomy. After graduation in 1865 from the University of Bern, Kocher spent a year visiting and studying at foreign clinics. He visited Glasgow, where he witnessed Lister’s revolutionary antisepsis work; Paris, where he met Louis Pasteur and Verneuil; and Zurich, where he met with Billroth. He became well versed in current developments in surgery. In 1872, at the age of 31, Kocher was appointed surgical chair at the University of Bern. Halsted observed that
a greater advance was made in the operative treatment of goiter in the decade from 1873 to 1883 than any in the forgone years, and I may say in all the years that have followed … during which period the art of operating for goiter by Billroth and Kocher and men of their school had been almost perfected, relatively minor problems remain to be solved.2
Figure 1-5 Theodor Kocher, 1912.
(Reproduced with permission from Institut für Medizingeschichte, Universität Bern, Buehlstrasse 26, CH 3012 Bern.)
At the time of Kocher’s appointment to Bern, goiters were endemic in Switzerland. Kocher noted that up to 90% of schoolchildren in Bern were afflicted with goiter.19 He quickly acquired a remarkable experience in thyroid surgery and eventually performed more than 5000 thyroidectomies over the course of his career. He was a meticulous surgeon who paid careful attention to hemostasis. He introduced initial ligation of the inferior thyroid arteries, which substantially reduced the risk of hemorrhage. His advocacy of the use of antisepsis and hemostasis, evident in his textbook of surgery, was manifest in his mortality rates. He reported a reduction in mortality from 12.6% in the 1870s to 0.2% in 1898.20 During Kocher’s tenure, Bern became the world capital of goiter surgery (Figure 1-6). Kocher’s surgical technique differed from Billroth’s in that Kocher preserved the strap muscles and usually used a collar incision, whereas Billroth typically used an oblique and more restrictive incision.13 Kocher also paid close attention to the anesthesia methods available. One of Kocher’s few mortalities was secondary to chloroform anesthesia. From that point onward, he used only local anesthesia with cocaine.8

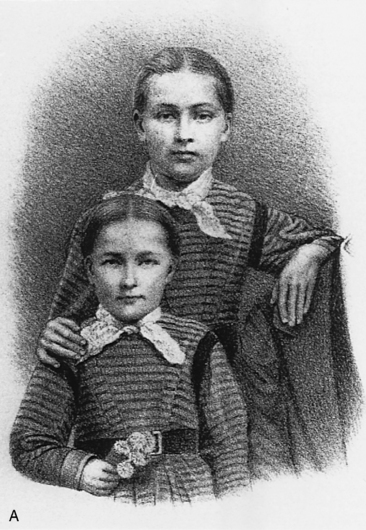
When Kocher, in 1882, became familiar with the work of Jaques-Louis Reveridin of Geneva, who described similar symptoms of myxedema after total thyroidectomy, he began a concerted effort to recall all his goiter patients.21 Of the 18 thyroidectomy patients Kocher was able to review, 16 displayed varying degrees of myxedema. Kocher was so appalled at the outcome epitomized by Marie Bischel (Figure 1-7) that he resolved never again to perform a total thyroidectomy for benign disease. This observation was the first evidence that the thyroid played a physiologic role in growth and development.

In 1883, Kocher presented his historic paper to the Fifth German Surgical Congress in which he described the adverse effects of total thyroidectomy (termed cachexia strumiprivia), evidence that the thyroid gland in fact had a function.22 About this time, Felix Semon, a Prussian otolaryngologist, in a meeting of the Clinical Society of London, also suggested similarities between English myxedematous patients and patients who had undergone total thyroidectomy.23,24
An interesting comparative observation between Billroth’s and Kocher’s surgical technique was made by William Halsted (Figure 1-8; see also Figure 1-6) who, as a student, visited the clinics of both.2 Halsted noted that most of Kocher’s thyroidectomy patients developed myxedema postoperatively, but rarely tetany. The reverse was true of Billroth’s patients. Halsted proposed that the origin of this phenomenon lay in Kocher’s and Billroth’s different surgical techniques. Whereas Kocher was known for his bloodless operative field, attention to detail, and removal of most of the thyroid while preserving surrounding structures, Billroth was known for a more rapid approach, resulting in parathyroid injury and larger retained segments of thyroid. Kocher was a versatile and astute surgeon whose accomplishments extended beyond that of endocrine surgery. Kocher’s achievements included the development of a method of shoulder dislocation reduction, use of the right subcostal incision in cholecystectomy, work with gunshot wounds and osteomyelitis, localization of spinal cord lesions, and development of the surgical mobilization maneuver of the duodenum that bears his name.13 In 1908, Kocher was awarded the Nobel Prize for his work on the physiology, pathology, and surgery of the thyroid gland. He has been acclaimed “the father of modern thyroid surgery.”3
Figure 1-8 William S. Halsted.
(From Organ CH Jr: J Am Coll Surg 191[3]:291, Fig. 11, 2000. Used with permission.)
William Halsted (1852-1922) (see Figure 1-8), a student and close acquaintance of Kocher, brought Kocher’s surgical philosophy to the American surgical arena. Following his graduation from Yale in 1879, Halsted studied for 2 years in well-known German and Austrian clinics, where he was influenced by the work of both Billroth and Kocher. On returning from Europe, Halsted was shocked at the state of thyroid surgery in the United States. In fact, little thyroid surgery was done at all in the United States at that time. In 1881, in New York, Halsted assisted Dr. Henry Sands at Roosevelt Hospital with resection of a right thyroid mass. The patient sat awake in a dental chair with a rubber bag tied around his neck to catch the blood. The two hemostats available at the hospital at that time were both used.3 Halsted was quick to utilize the knowledge of antisepsis and modern hemostatic forceps in the United States.4 In 1881, he wrote that the confidence “acquired from masterfulness in controlling hemorrhage gives to the surgeon the calm which is so needed for clear thinking and orderly procedure at the operative table.”2 His early work, however, was not without peril. While experimenting with local infiltration anesthetic agents, Halsted became addicted to cocaine.25 His work “The Operative Story of Goiter,” published in 1920, described advances made in thyroid surgery from the earliest days to the revolutionary work of Billroth and Kocher, whose techniques he held in great esteem.
Halsted helped to found the auspicious Johns Hopkins Hospital, where he was named the first Johns Hopkins professor of surgery. There he introduced residency training and trained many surgeons, including Cushing, Dandy, and Reed, and a number of respected thyroid surgeons, including Charles Horace, Frank Lahey, and George Crile.25 Crile’s contributions extended to early studies of shock and the surgical treatment of hyperthyroidism. Roswell Park used a pneumatic antishock suit, devised by Crile, to help prevent shock in hyperthyroid patients undergoing thyroid operations (Figure 1-9).
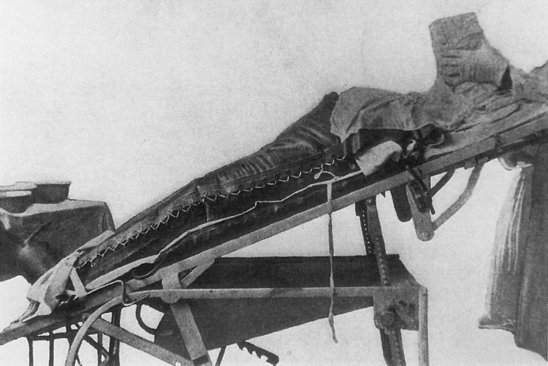
Figure 1-9 Crile’s pneumatic suit used to prevent shock in thyroid operations.
(From Park R. Principles and Practice of Modern Surgery, Philadelphia: Lea and Brothers; 1907. Used with permission.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


