Histopathology of Age-Related Macular Degeneration
Mariana Ingolotti
Eric P. Jablon
John Barnwell Kerrison
Hugo Quiroz-Mercado
D. Virgil Alfaro III
INTRODUCTION
Age-related macular degeneration (AMD) is the leading cause of central vision loss in the over-65 population in developed countries. It is a bilateral, degenerative, and chronic disease limited to the macula so that the peripheral retinal function is relatively preserved. Progressive histopathologic changes (Fig. 5.1) in the retinal pigment epithelium (RPE), retina photoreceptor cell layer, Bruch’s membrane (BM), and choriocapillaris are seen in these patients.
The most common histologic findings in nonneovascular or dry AMD are drusen; a thickened and basophilic BM; and geographic atrophy, hypertrophy, and hyperplasia of the RPE. Choroidal neovascularization (CNV), pigment epithelial detachment (PED), and disciform scar are important features of neovascular or wet AMD. The purpose of this chapter is to give a detailed description of the histopathologic findings encountered in AMD with emphasis on the ultrastructure, composition, and formation of different lesions.
NORMAL AGING OF THE RETINA
In discussing the histopathology of AMD, one must consider normal aging changes in the outer retina, a major risk factor for the development of this disease. The photoreceptor layer, RPE, BM, and choriocapillaris constitute the Ruysch’s complex (1). This complex suffers age-associated changes that commence at approximately the age of 20.
Certainly, the RPE shows ultrastructural changes seen in electron microscopy. Its melanin granules migrate to the basal portion of the cell, and the amount of lipofuscin granules increases as a result of the phagocytosis of the rod and cone outer segments. With age, the efficacy of rod and cone outer segment digestion reduces, and they can be extruded into the BM and in the space between the basement membrane of the RPE and its cellular membrane where they accumulate. Lipids from the digestion of organelles like mitochondria and endoplasmic reticulum can also deposit here (2).
Lipofuscin is an autofluorescent pigment formed through the oxidation of unsaturated fatty acids. In short, it is an undigestable residue of cytoplasmic catabolism. Studies showed that content of lipofuscin in the cells increases with age. On the contrary, melanin content decreases showing an inverse relation between these two compounds not only in their final concentration but also in their topographical distribution. This interesting finding may suggest a protective mechanism in the formation of lipofuscin (3).
Thickened BM is another alteration that occurs over time. Histologically, there is an increase in basophilia with hematoxylin and eosin (H&E) stain because of progressive calcium
salt and lipid deposition in both inner and outer collagenous zones (4). Moreover, studies have shown that a large portion of the lipids found in this tissue are lipoprotein-like particles that increase with advancing age. These deposits were found to increase in the inner collagenous and elastic layers, but not in the outer collagenous layer. Authors have related these findings to the formation of a hydrophobic barrier within the BM that altered the filtration capacity through the area (5). These deposits may also be related to small granules, another major deposit found at the BM by Huang et al. They suggested there could be an interaction between this two inclusion types, but the identity of these small granules could not be determined (6). In addition, the accumulation of cholesterol esters with advancing age can be compared to accumulation of cholesterol esters in the intima of large arteries in atherosclerosis (7). Finally, there is an increase in collagen cross-linking in the inner portion of this membrane causing a negative effect on its permeability. This cross-linkage provides strength and density to the collagen network together with the loss of flexibility, elasticity, and filtration properties. Therefore, the RPE collagenases become less effective in the removal of other BM components considering this tight network is blocking their way (8).
salt and lipid deposition in both inner and outer collagenous zones (4). Moreover, studies have shown that a large portion of the lipids found in this tissue are lipoprotein-like particles that increase with advancing age. These deposits were found to increase in the inner collagenous and elastic layers, but not in the outer collagenous layer. Authors have related these findings to the formation of a hydrophobic barrier within the BM that altered the filtration capacity through the area (5). These deposits may also be related to small granules, another major deposit found at the BM by Huang et al. They suggested there could be an interaction between this two inclusion types, but the identity of these small granules could not be determined (6). In addition, the accumulation of cholesterol esters with advancing age can be compared to accumulation of cholesterol esters in the intima of large arteries in atherosclerosis (7). Finally, there is an increase in collagen cross-linking in the inner portion of this membrane causing a negative effect on its permeability. This cross-linkage provides strength and density to the collagen network together with the loss of flexibility, elasticity, and filtration properties. Therefore, the RPE collagenases become less effective in the removal of other BM components considering this tight network is blocking their way (8).
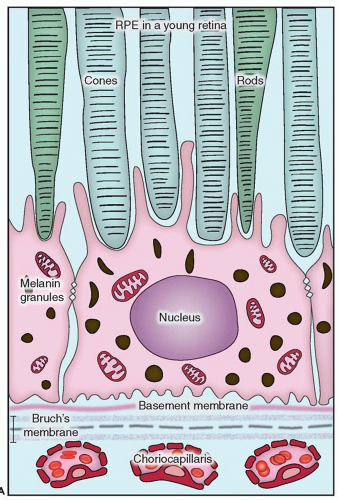 Figure 5.1 ▪ Histopathological changes in the two main forms of AMD. This diagram is showing the structural and functional changes of a normal RPE cell when developing dry or wet AMD. A. The RPE in a young retina has a homogenous distribution of the melanin granules, a BM without deposits, and a preserved function. |
The photoreceptor layer manifests a different response to aging. Immunohistochemical analysis concludes that the cone photoreceptor population shows more anomalies compared with rod photoreceptor population in non-AMD retinas. Nevertheless, the signs of degeneration have an early onset in cones, but rods appear to die more promptly. Cones can prolapse into the outer plexiform layer and
subretinal space and lose their synaptic contact without succumbing to cell death as do rods (9).
subretinal space and lose their synaptic contact without succumbing to cell death as do rods (9).
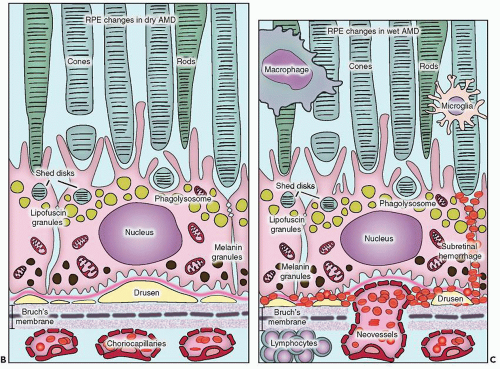 Figure 5.1 ▪ (Continued) B. In dry AMD, the RPE melanin granules are localized basally, and lipofuscin granules increase in number while the efficacy of the disks digestion reduces. Note the formation of drusen between the basement membrane of the RPE and the inner collagen layer of the BM and the thickened BM. C. In wet AMD, CNV develops, and an inflammatory response develops with an influx of lymphocytes and macrophages to the scene. These fragile new vessels leak and lead to subretinal hemorrhage. |
Some authors consider AMD to be an accentuation of normal aging changes. Age is a key factor in its pathogenesis. Nevertheless, many people maintain an excellent vision in spite of advancing age and its consequences.
DRY/NONNEOVASCULAR AMD
Drusen
Drusen are deposits of extracellular matrix localized between the basement membrane of the RPE and the inner collagen layer of the BM. They can extend to the outer collagenous zone if there is discontinuity in the central band of elastic fibers (10,11). They are often seen in the aging retina, as a hereditary condition (dominantly inherited drusen) or secondary to a variety of intraocular processes including inflammation, trauma, and chronic retinal detachment (2). However, an increase in number, size, and confluence was established as a risk factor for the development of AMD (12). Because of this, it is important to distinguish which yellow deposits will lead to atrophy of the RPE or CNV. The American Academy of Ophthalmology proposed the following classification according to the size of the drusen (13):
▪ Small (less than 64 µm of diameter)
▪ Intermediate (64-124 µm of diameter)
▪ Large (≥125 µm of diameter)
Immunohistochemical and proteomic studies of drusen composition have revealed different proteins other than RPE remnants (lipofuscin) like immunoglobulins, class II antigens, acute-phase proteins (e.g., fibrinogen, C-reactive protein, and vitronectin), components of the complement cascade and its inhibitors, apolipoproteins B and E, and lipids (e.g., cerebrosides), among others (8,14,15). These deposits are collectively known as drusen, but they are not all alike. Drusen main types are hard, soft, and diffuse or confluent, although authors have also described several others subtypes such as basal, nodular, mixed, and calcified regressing drusen (11).
Hard drusen are pinpoint-sized, sharp-edged yellowish retinal lesions easily seen on ophthalmoscopic exam. They are hyperfluorescent in the early stages of the fluorescein angiography and stain late without leakage. Histopathologically, hard drusen are hyaline-like, dense, rounded, homogenous bodies restricted to the basement membrane of the RPE and BM. They consist of a uniform periodic acid-Schiff-positive material and are eosinophilic on the H&E stain (Fig. 5.2A and B) until they start accumulating calcium and consequently become basophilic (16). They also stain lightly positive with special staining technique for lipid (2). On the electron microscopy, they are finely granular or amorphous nodules with similar electrodensity to the basal membrane of the RPE. They may also contain pale vesicles, tubular structures, curly membranes, and wide-banded collagen (15). The overlying RPE is thinned due to degenerative changes as described in Ulshafer et al. (17) electron microscopy studies. There are several hypotheses concerning the formation of hard drusen. Some authors have shown that the main initiating event in their development is the shedding of portions of RPE cells into the BM that are then hyalinized during the apoptosis process (18,19). Others have demonstrated that they are formed by lipidization and degeneration of single cells (20,21). This matter is still uncertain.
In contrast, soft drusen have less well-defined boundaries and tend to become confluent. Histologically, they are composed of a pale-staining amorphous more irregular and granular material located in the thickened inner layer of the BM. Green et al. (16) pointed out that they represent a serous detachment of the thickened inner aspect of the BM along with the RPE. On electron microscopy, this thickened area consists of vesicles, membranous debris, and wide-spaced collagen associated with the basal laminar deposits (22).
The basal deposits represent one of the earliest morphologic changes in the AMD. The two main types of basal deposits are basal laminar deposits (BLamDs) and basal linear deposits (BLinDs) (23). BLamDs are seen as soft granular eosinophilic material or extensive plaques that elevate the atrophic RPE from the inner surface of BM. On electron microscopy, these deposits are found to be limited to the plasma membrane and the basement membrane of the RPE and are comprised of extracellular matrix material with wide-spaced collagen (24). These deposits contain laminin, collagen type IV, vitronectin, extracellular matrix-modulating metalloproteinases, activated complement, glycoproteins, heparan sulfate, cholesterol, carbohydrates, and apolipoproteins B and E (8,25). In contrast, BLinDs are located in the thickened inner layer of the BM and appear to be electron dense rich in lipid material. These deposits represent what many authors have described as “diffuse drusen” (26). With progressive death of pigment epithelial cells, drusen start to fade by decreasing in size and becoming what some authors called calcified drusen (27




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
