Fig. 4.1
Typical myopic disc with tilting on fundus photograph. The disc appears oval with the maximal diameter along the vertical axis
Fig. 4.2
The schema of oblique insertion and disc tilting in high myopia. The optic nerve runs oblique to the eye wall, resulting in flattening of the temporal side and elevating of the nasal side
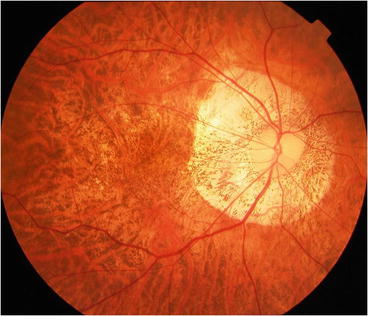
Fig. 4.3
A typical myopic macrodisc. The disc is not tilted, and unlike that in Fig. 4.1, this disc is flat with shallow cupping
A histomorphometric study reported that high myopic disc is about 1.5 times larger than non-myopic in absolute glaucoma [2], and fundus photographs show a substantially larger, and shallower disc in primary open-angle glaucoma with high myopia [3]. A large population study of Asian individuals reported that the disc area in myopic eyes is about 2–3 times larger than in emmetropic eyes and that the disc area is associated significantly with the degree of myopia. Interestingly, a graph of disc sizes showed a steep curve in high myopia, but the curve was relatively horizontal in moderate myopia, suggesting that the highly myopic disc has specific features among the different degrees of myopia [4].
4.3 Peripapillary Atrophy
4.3.1 Definition
The myopic temporal crescent, sometimes referred to as beta-zone peripapillary atrophy (PPA) and conus myopicus (myopic conus), is a white, sharply defined area on the temporal side of the optic disc where the inner scleral surface is directly observable (Fig. 4.4). The myopic temporal crescent results from displacement of the choroid and retinal pigment epithelium (RPE) because of protrusion of the posterior pole [1]. A larger area of PPA and a higher refractive error are highly correlated, and steep myopic increases exceeding −7 to −8 diopters have been reported [5], indicating that a large area of PPA is a hallmark of high myopia. There are two types of PPA. The first is a peripheral zone (alpha zone) characterized by irregular hypopigmentation and hyperpigmentation by fundus observation that is adjacent to the retina on the outer side; the second is the beta zone on the inner side, which is characterized by visible sclera and large choroidal vessels [6]. The myopic crescent normally presents temporal or inferotemporal to the disc and must be differentiated from the congenital tilted disc, which normally occurs inferiorly [7].
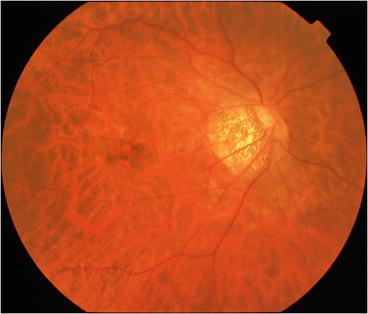
Fig. 4.4
The typical appearance of beta-peripapillary atrophy in high myopia. A whitish lesion with a well-defined border is seen that normally develops inferotemporal or temporal to the optic disc
4.3.2 Histological Observation
Histologically, the alpha zone corresponds to irregularities in the RPE, while the beta zones is characterized by complete loss of RPE cells and almost complete loss of photoreceptors and closure of the choriocapillaris [8].
Recently, gamma and delta zones also have been proposed based on the results of a histologic study of myopic eyes [9]. The gamma zone is between the end of Bruch’s membrane and the edge of the optic nerve head and was found predominantly in eyes with an axial length exceeding 26.5 mm, suggesting that the zone is specific to high myopia. The delta zone is part of the gamma zone in which blood vessels were not present. Interestingly, the length of the beta zone was not associated with high myopia but with glaucoma, while the lengths of the gamma and delta zones were associated with high myopia but not with glaucoma. We hypothesized that these proportional changes in the PPA zone may be associated with the susceptibility of the IOP in highly myopic eyes and may be why glaucoma develops in certain highly myopic eyes.
4.3.3 Optical Coherence Tomographic Findings
Some unique features within the area of PPA are specific to myopia or glaucoma. Spectral-domain optic coherence tomography (OCT) has shown that Bruch’s membrane is often absent within the beta-PPA area in highly myopic eyes. The scleral bed configurations within the PPA can be classified into three types based on OCT findings: straight, a downward curving Bruch’s membrane, or a downward bending slope without Bruch’s membrane. Only the last is associated significantly with the myopic refractive error, and interestingly, the second is associated significantly with glaucoma [10]. This fact suggests that the configuration of the scleral bed within the PPA is related closely to myopic glaucoma, which partly agrees with histologic observations [9].
New imaging modalities including SD-OCT provide detailed information about the anatomic relationships among the disc edge, Bruch’s membrane, and RPE. Observation using these new modalities has resulted in an argument that the beta-PPA should be redefined based on the findings using the latest generation of imaging tools. SD-OCT studies have found that the RPE was within the beta-PPA area in many cases, which is contrary to the initial definition based on histologic studies without RPE cells [11, 12].
4.3.4 Progression
The area of PPA enlarges over time with myopic progression (Fig. 4.5). The congenital crescent that normally does not enlarge must be ruled out. The myopic disc shifts nasally with axial length elongation, which induces myopic crescent development temporally. A follow-up study found a significant correlation between optic disc deviation and myopic progression [13].
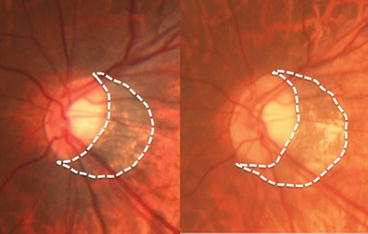
Fig. 4.5
Enlargement of peripapillary atrophy (PPA) over years. The same patient at baseline (left) and 10 years later (right); enlargement of PPA and increased disc tilting are seen (white dashed lines). The axial length has elongated from 28.67 mm to 29.03 mm
Serial disc photographs also showed progressive tilting of the optic nerve head with development or enlargement of the area of PPA in myopic children. In the group with changes in the optic nerve head and area of PPA, the mean horizontal-to-vertical disc diameter ratio decreased from 0.92 to 0.86, and the mean maximal PPA width-to-vertical disc diameter ratio increased from 0.08 to 0.20 during a mean follow-up period of 38.1 months. These changes were most marked in children between 7 and 9 years of age and were associated with a greater myopic shift [14]. Thus, a myopic shift induces disc tilting and consequent PPA enlargement in myopic eyes.
4.4 Tilted Disc
4.4.1 Ophthalmoscopic Appearance
Tilting is one of the most common features of a myopic disc; the nasal margin typically becomes elevated relative to the temporal margin. Angulation of the optic cup axis inferonasally is also common. Myopic discs with acquired crescents and congenital tilted discs can be difficult to distinguish because both have a severely attenuated RPE, Bruch’s membrane, and choroid close to the disc.
4.4.2 Relation to Myopia
Several studies have reported a positive association between tilted discs and long axial lengths. One study found that 55 of 150 myopic eyes had markedly tilted optic discs, with a cut-off value of the disc index less than 0.8. In addition, smaller disc ovality was observed in more highly myopic eyes with a longer axial length [15]. The relationship between optic disc tilt and myopia also has been reported in pediatric patients. Schoolchildren with tilted discs have significantly longer axial lengths and greater myopic refractive errors [16].
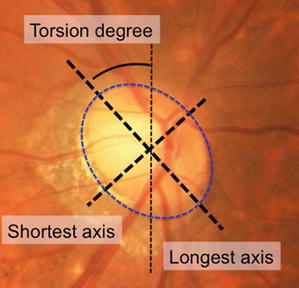
4.4.3 Conventional Indices for Tilted Discs
Because the maximal angle of the disc tilting cannot be measured directly, it is estimated by the degree of disc ovality (Fig. 4.6). When viewed along the visual axis, the less perpendicular the optic nerve is when it enters the globe, the greater the elliptical appearance is. The papillary index, defined by the shortest axis/longest axis on fundus photographs, has been used as the gold standard to represent the degree of disc tilting [17]. The threshold to define the tilted disc often is lower than 0.8–0.75. Non-myopic discs are minimally oval with the vertical diameter slightly longer than the horizontal, and the index is close to 1.0.