Complications, risks, and consequences
Estimated frequency
Most significant/serious complications
Bruising
50–80 %
Bleeding/hematoma formationa
5–20 %
Infection
1–5 %
Seroma formation
5–20 %
Rare significant/serious problems
Suture abscess ± suture sinusa
0.1–1 %
Hernia recurrencea
0.1–1 %
Laparotomy (bowel injury or adhesion related strangulation)a
0.1–1 %
Dehiscence
<0.1 %
Less serious complications
Pain/discomfort/tenderness
Acute (<4 weeks)
20–50 %
Chronic (>12 weeks)
0.1–1 %
Scarring
1–5 %
Dimpling/deformity of the skina
1–5 %
Numbness/altered sensation
1–5 %
Drain tube(s)a
1–5 %
Perspective
Most symptomatic epigastric hernias cause discomfort rather than bowel obstruction. Because of the narrow defect in some cases, chronic incarceration of pre-peritoneal fat is not uncommon, and these herniae are irreducible. The risk of infection is increased when bowel is obstructed. If bowel obstruction is present, the offending loop must be visualized and its viability assessed at the time of repair. This may require extension of the incision or conversion to full laparotomy to assess bowel viability. The usual complications associated with abdominal wall surgery are seen. Monofilament, nonabsorbable suture is usually used to repair the defect. Plastic mesh is sometimes used; however, this slightly increases the risk of foreign body reactions and infection. To date, recurrence rates have not been formally assessed in prospective trials, but are generally considered to be infrequent.
Major Complications
Infections are mainly of skin (Staphylococcus aureus) origin; however, bowel derived organisms (Escherichia coli; bacteroides sp.; Strep pyogenes) may be causative when bowel is obstructed or breached. Infection often necessitates removal of some, or all, foreign material such as sutures and mesh and may dictate later hernia repair. Infection also increases the risk of suture sinus, dehiscence, and hernia recurrence. Bleeding may occur from vessels associated with the edge of the peritoneal hernial sac, and especially from omental vessels that are often thin walled and easily traumatized. Occasionally, mesenteric vessels can be traumatized during reduction of bowel causing bleeding. These situations do not usually present difficulty in obtaining control of bleeding. Bowel Injury is a potentially serious problem and can occur easily if ischemia and/or infarction of bowel is present. Extension of the incision or midline conventional laparotomy is often safest to fully inspect the bowel. Occasionally perforation has occurred and infection is established before surgery. This can present some difficulty with regard to repair using a nonabsorbable suture or mesh. However, mass closure using monofilament sutures is usually satisfactory. Avoidance of mesh, or any foreign material that is more than absolutely necessary for closure, is advisable. Rarely, delayed primary closure is indicated, with subsequent delayed elective hernia repair some months later. Suture Sinus may develop as a result of a foreign body reaction to suture material, especially knots, or mesh. Infection can cause, or be secondary to, suture sinuses. When established, a suture sinus will usually only settle after removal of the offending foreign material. However, removal of some of the material may be sufficient, and then the main bulk of material used in the repair can be retained. Sometimes, however, all foreign material has to be removed to heal the sinus and/or infection. There is a small incidence of hernia recurrence after repair, and although patients should be warned about this, it is usually not problematic in most cases. Seroma Formation produces a lump, which usually resorbes spontaneously and settles and may need needle aspiration drainage(s) to assist this. However, needle aspiration may increase the risk of secondary infection.
Consent and Risk Reduction
Main Points to Explain
Discomfort
Bleeding
Infection
Bowel perforation
Recurrent hernia
Laparotomy
Further surgery
Risks without surgery
Surgery for Umbilical/Paraumbilical Hernia
Description
General anesthesia is usually used; however local infiltration and high spinal anesthesia can be used in selected cases, with or without systemic neuroleptic agents. One or multiple defects may be present. The aim of the procedure is to define the sac(s), then excise and repair the defect(s). A transverse skin incision either below or above the umbilicus is usually used. Rarely a longitudinal midline incision is utilized. Umbilical and paraumbilical hernias (UH/PUH) are relatively common surgical problems that spans the ages and sexes in nearly equal frequency. Umbilical herniae are through the embryological physiological defect at the umbilical cord where the expanding gut tube herniates and returns to the abdominal cavity by 10 weeks of gestation. Umbilical herniae are common at birth and usually close by the age of 2 years. Many adults have these as persistent umbilical defects, but are never aware of this until pointed out by a surgeon. Paraumbilical herniae are usually defined as acquired defects in the abdominal wall cicatrix adjacent to the umbilicus, but many regard this distinction as somewhat artificial. In essence, both umbilical and paraumbilical herniae are managed surgically the same way. The herniae have a peritoneal sac usually containing omentum. Less commonly bowel may herniate, particularly in larger herniae. In obese patients, the diagnosis may be especially difficult. Most UH/PUH are reducible using gentle compression and a finger can often be inserted into the hernial defect inverting the skin and sac to palpate a “cough impulse” as the patient coughs. The hernia is usually rapidly re-created after the examining finger is removed and the patient coughs again. Elective repair is indicated in symptomatic patients; incarceration and bowel obstruction require emergency intervention. Since there is a greater risk of bowel herniation in UH/PUH, than epigastric hernia, there is a tendency to recommend surgical repair for UH/PUH. The sac is defined and excised at the edge of the linea defect, and from the overlying skin of the umbilicus, to expose the contents before reduction. A midline longitudinal incision through the linea alba above and/or below the UH/PUH defect is usual to extend the hernial opening, if better access is needed to reduce or inspect the hernial contents. The defect is closed usually using nonabsorbable monofilament sutures, either interrupted or continuous, or a combination; however, many surgeons use mesh, depending on the size and physical demands of the patient. Recurrent hernias often require mesh. The subcutaneous tissues are closed with an absorbable suture and skin closed with a continuous subcuticular suture or staples.
Anatomical Points
Additional defects should be sought at the time of repair because there may be associated midline abnormalities or fascial defects lateral to the midline at the umbilicus. Missing these at the initial operation leads to an apparent increased “recurrence” rate (actually separate herniae). To avoid this event digital or visual exploration of the midline at least 10 cm around the umbilicus is advocated to detect a synchronous herniae; if present, repair is needed to avoid the risk of a “recurrence” (Table 6.2).
Table 6.2
Surgery for umbilical/paraumbilical hernia estimated frequency of complications, risks, and consequences
Complications, risks, and consequences | Estimated frequency |
|---|---|
Most significant/serious complications | |
Bruising (including minor and severe) | >80 % |
Bleeding/hematoma formationa | 5–20 % |
Seroma formation | 5–20 % |
Infection | 1–5 % |
Rare significant/serious problems | |
Laparotomy (bowel injury or adhesion related strangulation)a | 0.1–1 % |
Hernia recurrencea (10 year) | 0.1–1 % |
Dehiscence | <0.1 % |
Less serious complications | |
Pain/discomfort/tenderness | |
Acute (<4 weeks) | 20–50 % |
Chronic (>12 weeks) | 0.1–1 % |
Dimpling/deformity of the Skina | 1–5 % |
Numbness/altered sensation | 1–5 % |
Scarring | 1–5 % |
Suture abscess ± suture sinusa | 0.1–1 % |
Drain tube(s)a | 1–5 % |
Perspective
The complications related to UH/PUH repair are generally not major, but in certain situations infection and bleeding can be problematic. At times, the defect must be enlarged to effect reduction and inspection of the contents and in that situation mesh should be considered an element in the repair. Numbness and injury to nerves is not likely in this procedure given the anatomy and innervation of the central abdominal wall. However, discomfort can persist for some time in some patients and may be a source of dissatisfaction. Occasionally, especially after weight loss, the suture ends or mesh can become palpable and irritating; however, this is partly determined by surgical technique. Repair using laparoscopic techniques produces a different distribution of complications associated with the risks to intra-abdominal organs from laparoscopic entry into the abdomen. Hernia recurrence is related to the quality of the patient’s tissues and surgical technique.
Major Complications
Infection is not usually a problem; however, skin organisms predominate unless bowel injury has occurred. The use of mesh or nonabsorbable sutures may engender bacterial colonization and increase the risk of infection slightly. Wound dehiscence is rare. Bleeding is seldom severe unless an omental or mesenteric vessel is transected, especially at the edge of the peritoneal hernial sac, and from omental vessels that are often thin walled and easily traumatized. The porto-systemic venous anastomoses around the umbilicus can produce annoying bleeding, but in rare patients with portal hypertension, bleeding can be substantial and greater care must be taken. Occasionally, mesenteric vessels can be traumatized during reduction of bowel causing bleeding. These situations do not usually present difficulty in obtaining control of bleeding. Fluid leakage, and particularly ascitic leakage is more of a problem in patients with established ascites. Bowel injury is a potentially serious problem and can occur easily if ischemia and/or infarction of bowel is present. Extension of the incision or midline conventional laparotomy is often safest to fully inspect the bowel, if required. Occasionally perforation has occurred and infection is established before surgery. This can present some difficulty with regard to repair using a nonabsorbable suture or mesh. However, mass closure using monofilament sutures is usually satisfactory. Avoidance of mesh, or any foreign material that is more than absolutely necessary for closure, is advisable in situations of bowel perforation. Rarely, delayed primary closure is indicated, with subsequent delayed elective hernia repair some months later. Suture Sinus may develop as a result of a foreign body reaction to suture material, especially knots, or mesh. Infection can cause, or be secondary to, suture sinuses. When established, a suture sinus will usually only settle after removal of the offending foreign material. However, removal of some of the material may be sufficient, and then the main bulk of material used in the repair can be retained. Sometimes, however, all foreign material has to be removed to heal the sinus and/or infection. Hernia recurrence rates for these hernia repair complications are rather high and further increased in the presence of obesity. The use of prosthetic mesh in the repair is advocated if the defect exceeds 3 cm in diameter, the tissues are weak or likely to be repeatedly stressed. Placement of the mesh below the rectus fascia and above the peritoneum has been advocated to minimize recurrence, but placement superficial to the fascia is also successful. Weakened tissues are a major reason for initial herniation and also for recurrence.
Consent and Risk Reduction
Main Points to Explain
Discomfort
Bleeding
Infection
Bowel perforation
Recurrent hernia
Laparotomy
Further surgery
Risks without surgery
Surgery for Primary Open Inguinal Hernia
Description
Open inguinal hernia repair can be performed under general, local, or regional (spinal or epidural block) anesthesia. The aim is to define and locate the type (direct, indirect, or both) of inguinal hernia and repair it. A lower abdominal or groin transverse incision is often used, however, an oblique incision is sometimes preferred; both afford good access. Inguinal herniae occur through the anterior abdominal wall via the deep inguinal ring (indirect) or a nonphysiological defect in the transversalis fascia medially (direct) or occasionally both (see anatomy). The defect is closed usually using nonabsorbable monofilament sutures, either interrupted or continuous, or a combination; however, many surgeons use mesh, depending on the size and physical demands of the patient. The subcutaneous tissues are closed with an absorbable suture and skin closed with a continuous subcuticular suture or staples.
Anatomical Points
Indirect inguinal herniae occur through the physiological defect at the deep inguinal ring traveling along the spermatic cord in the male, or the “gubernaculum” in the female. Direct inguinal herniae are nonphysiological defects “directly” through the transversalis fascia. Indirect herniae arise laterally, and direct herniae arise medially, to the inferior epigastric vessels; however, the main hernia mass may lie anywhere along the inguinal canal. Indirect herniae may extend into the scrotum. The size of the defect can vary widely for both types of hernia and both may coexist as a complex or “pantaloon” type hernia, protruding either side of the inferior epigastric vessels. The hernial mass comprises a sac containing fluid, peritoneal and/or omental fat, bowel or bladder. Rarely the appendix or ovary may be included. Because direct herniae are more medially placed, bladder is more often included. The position of the ilioinguinal nerve is highly variable sometimes branching early and can be difficult to identify, increasing its risk of injury. Usually, it overlies the spermatic cord, but may be displaced by the hernia. Varicosities of the spermatic (testicular) veins may make dissection of the hernial sac difficult, increasing the risk of bleeding. Chronic scarring of the sac may also distort the anatomy. The cremaster muscle may be extensive, requiring ligation and excision to permit proper access for repair (Table 6.3).
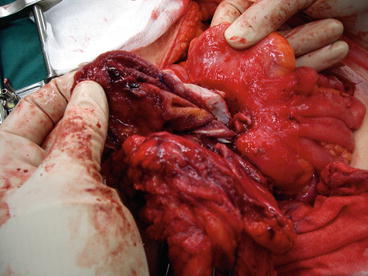
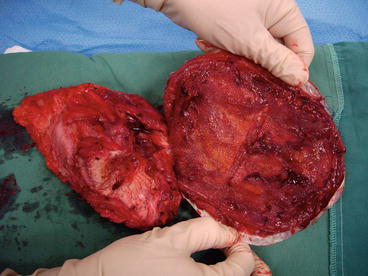



Fig. 6.6
Infected abdominal incisional hernia mesh
Fig. 6.7
Infected abdominal incisional hernia mesh removed
Fig. 6.8
Vacuum dressing in place
Fig. 6.9
Healing wound after vacuum dressing
Fig. 6.10
Wound sinus infected mesh
Table 6.3
Surgery for open inguinal hernia estimated frequency of complications, risks, and consequences
Complications, risks, and consequences | Estimated frequency |
|---|---|
Most significant/serious complications | |
Bruising | 50–80 % |
Bleeding or hematoma formationa | 1–5 % |
Infectiona | 0.1–1 % |
Seroma formation | 1–5 % |
Numbness/altered sensation | 1–5 % |
Neural injurya | |
Ilioinguinal nerve | 1–5 % |
Iliohypogastric nerve | 1–5 % |
Hernia recurrencea (10 year) | 1–5 % |
Rare significant/serious problems | |
Vascular injury—artery or vein | 0.1–1 % |
Arterial injury | 0.1–1 % |
Constriction of femoral vein | <0.1 % |
Deep venous thrombosis | 0.1–1 % |
Suture abscess/granuloma formation ± suture sinusa | 0.1–1 % |
Spermatic cord injurya | 0.1–1 % |
Testicular ischemia, testicular atrophy | 0.1–1 % |
Testicular necrosis/orchidectomy (rare in repair of primary inguinal hernias) | <0.1 % |
Small bowel obstruction | 0.1–1 % |
Laparotomy (bowel injury or adhesion related strangulation or ischemia)a | 0.1–1 % |
Dehiscence | <0.1 % |
Injury to femoral nerve | <0.1 % |
Less serious complications | |
Pain/discomfort/tenderness (wound/testicular/thigh pain)a | |
Acute (<4 weeks) | 20–50 % |
Chronic (>12 weeks) | 0.1–1 % |
Wound scarring (all) | 1–5 % |
Dimpling/deformity of the skina | 0.1–1 % |
Scrotal/labial swelling | 5–20 % |
Urinary retention | 1–5 % |
Drain tube(s)a | 1–5 % |
Perspective
Quantification of the complications associated with open repair of inguinal hernias is difficult for many reasons related to the underreporting of complications as for many surgical procedures. Infection, bleeding, and bowel injury are the major complications of note. Laparotomy for bowel iatrogenic injury is very rare and stoma formation because of this even more rare, but both are reported. It is more commonly associated with bowel incarceration and infarction. Given the number of hernia repairs done annually around the world, and the number of surgeons performing these repairs, it is expected that the results will vary from center to center. A few randomized trials of sufficient size have managed to establish reference values for most of the complications seen in open groin hernia repair. Of course, the wide variety of repairs available will not have the same complication rates; however, some complications will be common and others unique to the specific repair. Hence the rather broad range of frequencies for each of the “common” complications noted. Some readers will perceive some of the values to be too high based on their experience. Many of the complications are indeed rare and clearly relate to the specific technique or repair employed. Modern surgical training has all but eliminated the spermatic cord, testicular and vascular injury noted in the past, reducing these to the relatively rare range when in the past these figures were considerably higher. More modern studies have looked at post-hernia repair pain, now reported as high as 50 % in some prospective studies; it is considered a major issue. Indeed, there appears to be a significant increase in the incidence of post-repair chronic pain that is not entirely understood and may be related to the use of prosthetic mesh as the primary basis for the repair. Only recently true recurrence rates have been appreciated for the various anterior repairs and they all are in the 1–2 % range, independent of technique. When discussing recurrence rates it is important to note that many patients with recurrence appear years after the repair and recurrence rates at 10 and 20 years are yet to be established for many of the more common repairs in use today. Acute hernia repair failure, within days to weeks is likely to be underreported. With the introduction of the tension free approach to the repair of groin hernia, acute failures are rare. There is variation depending on the individual, center or site reporting their experience; however, there is an apparent increase in the incidence of chronic pain associated with this repair dependent on the intensity of investigation.
Major Complications
Infection is chiefly from skin (S. aureus) origin. Bowel derived organisms (E. coli; bacteroides sp.; Strep pyogenes) may be causative when bowel is obstructed or breached. Infection often necessitates removal of some, or all, foreign material such as sutures and mesh and may dictate later hernia repair. Infection also increases the risk of suture sinus, dehiscence, and hernia recurrence. Bleeding may occur from vessels associated with the edge of the peritoneal hernial sac, including the inferior epigastric vessels, outside the sac. Within the sac, the omental vessels are often thin walled and easily traumatized and occasionally mesenteric vessels can be traumatized during reduction of bowel, causing bleeding. Testicular or cremasteric vessels may also bleed. These situations do not usually present difficulty in obtaining control of bleeding. Bowel Injury is a potentially serious problem and can occur easily if ischemia and/or infarction of bowel is present due to incarceration and strangulation. Conventional midline laparotomy, or perhaps lateral incision of the deep ring, is often safest to fully inspect the bowel, if needed. Occasionally, perforation has occurred before surgery and infection is established. This can present some difficulty with regard to repair using any nonabsorbable suture. Avoidance of mesh, or any foreign material that is more than absolutely necessary for closure, is advisable. Delayed primary closure may be then indicated, with subsequent delayed elective hernia repair some months later. However, in special cases mass closure using monofilament sutures might still be performed. Suture Sinus may develop as a result of a foreign body reaction to suture material, especially knots, or mesh. Infection may either cause, or be secondary to suture sinuses. When established, a suture sinus will usually only settle after removal of the offending foreign material. However, removal of only some of the material may be required and frequently the main bulk of material used in the repair can be retained if granulation of tissue occurs over the mesh. Sometimes, however, all foreign material has to be removed to heal the sinus and/or infection. There is a small incidence of hernia recurrence after repair, and although patients should be warned about this, it is usually not problematic in most cases. The recurrence rate increases with the time observed and after infection-related hernia complications.
Consent and Risk Reduction
Main Points to Explain
Discomfort
Bleeding
Infection
Bowel perforation
Recurrent hernia
Laparotomy
Further surgery
Risks without surgery
Surgery for Recurrent Open Inguinal Hernia
Description
Recurrent open inguinal hernia repair can be performed under general, local, or regional (spinal or epidural block) anesthesia. The aim is to define and repair the recurrent hernia, usually using monofilament suture material or mesh. A lower abdominal or groin transverse or oblique incision is often used, and typically the old scar from the previous repair(s) is excised, if that is appropriate. Recurrent inguinal herniae can occur through the anterior abdominal wall via the same or a different defect at the deep inguinal ring (indirect) or in the transversalis fascia (direct) (see anatomy). Direct inguinal hernia “recurrence” is more common. Recurrent indirect inguinal herniae after a technically correct ligation of an indirect sac and repair should be very rare; however, occasionally an indirect sac is not detected at operation for a direct hernia. Recurrence of a direct hernia at the medial end of an indirect hernia repair is the commonest reported recurrent inguinal hernia site. This probably arises from failure to continue the repair sufficiently far enough medially, and/or recurrently weakened tissues. The defect is closed usually using nonabsorbable monofilament sutures, either interrupted or continuous, or a combination; however, many surgeons use mesh, depending on the size and physical demands of the patient. Recurrent hernias often require mesh. The subcutaneous tissues are closed with an absorbable suture and skin closed with a continuous subcuticular suture or staples.
Anatomical Points
Recurrent inguinal herniae usually occur directly through a nonphysiological defect in the transversalis fascia (direct hernia), but can occur through the physiological defect at the deep inguinal ring (indirect hernia) traveling along the spermatic cord in the male, or the gubernaculum in the female. Indirect herniae arise laterally and direct herniae arise medially to the inferior epigastric vessels; however, the main hernia mass may lie anywhere along the inguinal canal. Indirect herniae may extend into the scrotum. The size of the defect can vary widely for both types of hernia and both may coexist as a complex or “pantaloon” type hernia, either side of the inferior epigastric vessels. The hernial mass comprises a sac containing fluid, peritoneal and/or omental fat, bowel or bladder. Rarely the appendix or ovary may be included. Because direct herniae are more medially placed, bladder is more often included. The position of the ilioinguinal nerve is highly variable and this may branch early and can be difficult to identify, increasing the risk of injury, especially so for recurrent herniae due to scarring. Usually it overlies the spermatic cord, but may be displaced by the hernia or scar tissue. Varicosities of the spermatic (testicular) veins may make dissection of the hernial sac difficult, and entrapment of testicular vessels in scar tissue can increase the risk bleeding and testicular ischemia. Chronic scarring from previous surgery may also distort the anatomy. The cremaster muscle may be extensive, requiring ligation and excision to permit proper access for repair (Table 6.4).
Table 6.4
Surgery for recurrent open inguinal hernia estimated frequency of complications, risks, and consequences
Complications, risks, and consequences | Estimated frequency |
|---|---|
Most significant/serious complications | |
Bruising | 50–80 % |
Bleeding/hematoma formationa | 1–5 % |
Infectiona | 0.1–1 % |
Seroma formation | 5–20 % |
Numbness/altered sensation | 1–5 % |
Neural injurya | |
Ilioinguinal nerve | 5–20 % |
Iliohypogastric nerve | 5–20 % |
Ilioinguinal, iliohypogastric, genitofemoral nerve paresthesiaa | 20–50 % |
Hernia recurrencea (10 year) | 1–5 % |
Rare significant/serious problems | |
Femoral nerve paresthesia (if femoral nerve block used)a | 0.1–1 % |
Vascular injury—artery or vein | 0.1–1 % |
Constriction of femoral vein | <0.1 % |
Arterial injury | 0.1–1 % |
Deep venous thrombosis | 0.1–1 % |
Suture abscess/granuloma formation ± suture sinusa | 0.1–1 % |
Spermatic cord injurya | 0.1–1 % |
Testicular ischemia, testicular atrophy | 0.1–1 % |
Testicular necrosis/orchidectomy (rare in repair of primary inguinal hernias) | <0.1 % |
Small bowel obstruction | 0.1–1 % |
Laparotomy (bowel injury or adhesion related strangulation or ischemia)a | 0.1–1 % |
Fecal fistula | <0.1 % |
Urinary fistula | <0.1 % |
Dehiscence | <0.1 % |
Injury to femoral nerve | <0.1 % |
Less serious complications | |
Pain/discomfort/tenderness (wound/testicular/thigh pain)a | |
Acute (<4 weeks) | 20–50 % |
Chronic (>12 weeks) | 0.1–1 % |
Scrotal/labial swelling | 5–20 % |
Wound scarring | 1–5 % |
Urinary retention | 1–5 % |
Dimpling/deformity of the skina | 1–5 % |
Wound scarring | 1–5 % |
Drain tube(s)a | 1–5 % |
Perspective
There are many potential complications associated with open repair for recurrent groin herniae. Many are related to the specific techniques and approaches used for both the original and recurrent hernia repairs. Anterior or posterior/pre-peritoneal approaches with or without mesh can be used. Previous anterior repairs often leave scarring making a repeat anterior approach more dangerous for injury to the testicular vessels and vas deferens. The posterior approach often offers better-defined tissue planes and minimal scarring, reducing risk. The posterior approach has the advantage of dissecting through relatively unscarred tissues. In 800 cases, the recurrence rate for first-time recurrent groin hernia was 1.6 %, and for multiply recurrent defects about 3.5 % at 5 years. Similar results have been reported recently from randomized trials. Surgeon’s experience is a key factor in minimizing complications associated with the repair of any recurrent hernia independent of the approach selected. Working in the pre-peritoneal space demands the experience and an appreciation of the anatomy in order to effect a complete repair of all the defects found. Injury to peripheral nerves, ilioinguinal, iliohypogastric, and iliofemoral is seen more frequently with the anterior repair of recurrent hernias. Chronic groin pain after surgery for recurrent inguinal herniae is not uncommon. In a detailed analysis of recurrent hernia defects defined at the time of pre-peritoneal repair, 15 % of the defects were classified as complex or multiple, often unsuspected preoperatively, supporting the posterior approach for repair of these hernias. The posterior approach affords complete visual access to the entire inguinal floor and thus allows definition of all defects so that complete repair is possible. There are increased risks of injury to bowel, bladder, or vessels if one is not familiar with the anatomy. The laparoscopic approach to the repair of recurrent groin hernia—predicated on the posterior approach—has a slightly higher reported incidence of early failure and nerve and vessel injury. Avoiding the major complications in the repair of recurrent groin hernias reflects training, care, experience, and judgement, with each of the latter a function of the former.
Major Complications
Infection is mainly of skin (S. aureus) origin. Bowel derived organisms (E. coli; bacteroides sp.; Strep pyogenes) may be causative when bowel is obstructed or breached. Infection often necessitates removal of some, or all, foreign material such as sutures and mesh and may dictate later hernia repair. Infection also increases the risk of suture sinus, dehiscence, and hernia recurrence. Bleeding may occur from vessels associated with the edge of the peritoneal hernial sac, including the inferior epigastric vessels, outside the sac. Within the sac, the omental vessels are often thin walled and easily traumatized and occasionally mesenteric vessels can be traumatized during reduction of bowel, causing bleeding. Testicular or cremasteric vessels may also bleed. These situations do not usually present difficulty in obtaining control of bleeding. Bowel injury is a potentially serious problem and can occur easily if ischemia and/or infarction of bowel is present due to incarceration and strangulation. Conventional midline laparotomy, or perhaps lateral incision of the deep ring, is often safest to fully inspect the bowel. Occasionally perforation has occurred before surgery and infection is established. This can present some difficulty with regard to repair using any nonabsorbable suture. Avoidance of mesh, or any foreign material that is more than absolutely necessary for closure, is advisable. Delayed primary closure may be then indicated, with subsequent delayed elective hernia repair some months later. However, in special cases mass closure using monofilament sutures might still be performed. Testicular injury is not uncommon during recurrent inguinal hernia repair, especially with a repeated anterior approach, due to dense scar tissue and/or mesh entrapping the testicular blood supply and cord. Vascular injury causes testicular ischemia, and if sufficient may necessitate orchidectomy. Suture sinus may develop as a result of a foreign body reaction to suture material, especially knots, or mesh. Infection may either cause, or be secondary to suture sinuses. When established, a suture sinus will usually only settle after removal of the offending foreign material. However, removal of only some of the material may be required and frequently the main bulk of material used in the repair can be retained if granulation of tissue occurs over the mesh. Sometimes, however, all foreign material has to be removed to heal the sinus and/or infection. There is a recognized incidence of hernia recurrence after repeat hernia repair, and although patients should be warned about this, it is usually not problematic in most cases. The recurrence rate is time dependent. The factors that have lead to one recurrence, such as weak tissues may contribute to further recurrences.
Consent and Risk Reduction
Main Points to Explain
Discomfort
Bleeding
Infection
Bowel perforation
Recurrent hernia
Laparotomy
Testicular injury/removal
Further surgery
Risks without surgery
Surgery for Laparoscopic Hernia Repair (Pre-Peritoneal Approach)
Description
Laparoscopic TEP approach to inguinal hernia repair is performed under general anesthesia. Inguinal herniae occur through the anterior abdominal wall via the deep inguinal ring or a nonphysiological defect in the transversalis fascia (see anatomy). Laparoscopic approaches are also increasingly used for recurrent or bilateral hernia repairs.
Anatomical Points
Indirect inguinal herniae occur through the physiological defect at the deep inguinal ring traveling along the spermatic cord in the male, or the gubernaculum in the female. Direct inguinal herniae are nonphysiological defects “directly” through the transversalis fascia. Indirect herniae arise laterally and direct herniae arise medially to the inferior epigastric vessels; however, the main hernia mass may lie anywhere along the inguinal canal. Indirect herniae may extend into the scrotum. The size of the defect can vary widely for both types of hernia and both may coexist as a complex or “pantaloon” type hernia, protruding either side of the inferior epigastric vessels. The hernial mass comprises a sac containing fluid, peritoneal and/or omental fat, bowel or bladder. Rarely the appendix or ovary may be included. Because direct herniae are more medially placed, bladder is more often included. Varicosities of the spermatic (testicular) veins may make dissection of the hernial sac difficult, increasing the risk of bleeding. Chronic scarring of the sac may also distort the anatomy. Adequate definition of the anatomy is important (Table 6.5).
Table 6.5
Surgery for laparoscopic (pre-peritoneal approach) estimated frequency of complications, risks, and consequences
Complications, risks, and consequences | Estimated frequency |
|---|---|
Most significant/serious complications | |
Bleeding/hematoma formationa | 1–5 % |
Hernia recurrencea (5 year) | 1–5 % |
Injury to ilioinguinal nerve | 1–5 % |
Spermatic cord injury (overall)a | 1–5 % |
Testicular ischemia, testicular atrophy | 1–5 % |
Testicular necrosis/orchidectomy (rare in repair of primary inguinal hernias)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

| |