Complications, risks, and consequences
Estimated frequency
Most significant/serious complications
Infection
1–5 %
Bleeding/hematoma formation
1–5 %
Vascular injury
1–5 %
External jugular vein branches
Thyroid injurya
1–5 %
Damage to endotracheal tube/cuff
1–5 %
Respiratory obstruction
Early or late
1–5 %
Rare significant/serious problems
Tracheal necrosisa
0.1–1 %
Tracheal stenosisa
0.1–1 %
Tracheomalaciaa
0.1–1 %
Neural injury
0.1–1 %
Recurrent laryngeal nerve (X)
Cervical plexusa
Surgical emphysema (major)
0.1–1 %
Tracheal rupture
<0.1 %
Persistent or recurrent cyst/sinus/fistula
<0.1 %
Less serious complications
Pain or tenderness (sore throat; sore neck—transient)
Acute (<4 weeks)
>80 %
Chronic (>12 weeks)
1–5 %
Numbness/altered sensation
1–5 %
Bruising
50–80 %
Dimpling/deformity of the skin
1–5 %
Flap (skin) necrosis (significant)
0.1–1 %
Wound scarring (poor cosmetic result)a
1–5 %
Perspective
The major risk and debility potentially resulting from percutaneous needle mini-tracheostomy surgery is bleeding. This may occasionally lead to a hematoma formation, rarely large enough to require surgical evacuation and hemostasis. Skin necrosis is often very minor and heals spontaneously or with limited dressings. Skin grafts or flaps are rarely required. Infection can rarely be significant. Respiratory obstruction is a potential problem (1) at entry to the trachea as the tracheostomy tube is inserted as the endotracheal tube is withdrawn, (2) later if the endotracheal tube dislodges, (3) at the time of tube changes, or (4) from blood clot or mucus plug obstruction. Excessive cuff pressure may lead to ulceration and tracheal necrosis. Tracheomalacia causes decreased rigidity of the cartilage in the trachea and tracheal collapse. Tracheal stenosis may result from fibrosis/scarring of the tracheal wall. Cosmetic deformity at the tracheostomy site in the central lower neck is common. Accidental puncture of other neck structures: vessels and esophagus, and thyroid tissue can occur, as can tube dislodgement and surgical emphysema.
Major Complications
The most serious complications can arise from tracheal tube dislodgement causing respiratory obstruction, or damage to the trachea. Oxygen desaturation at the time of tracheostomy tube insertion can be a major issue if the airway is not maintained. Pre-oxgenation prior to tube insertion/manipulation is helpful in providing more safety and time. Bleeding may be significant and reduce vision and difficulty with placement of the tube into the trachea. Infection is rarely severe, but chronic purulent discharge around the tracheostomy tube entry site is not uncommon. Abscess formation and systemic sepsis are very rare. Surgical emphysema is rarely severe and due to air-leak around the tube into the tissues. Tracheal ulceration and necrosis may arise form excessive cuff pressure and prolonged tracheostomy or prior endotracheal intubation. Tracheal rupture is very rare. Tracheal stenosis may arise from fibrosis and scarring resulting from tracheal ulceration or necrosis. Cosmetic deformity from the indrawn scar is not uncommon and can be surgically corrected later, but needs to be balanced against the necessity for a tracheostomy.
Consent and Risk Reduction
Main Points to Explain
GA risk
Respiratory obstruction
Bleeding/hematoma
Wound infection
Abscess formation
Cosmetic deformity
Further surgery
Open Tracheostomy
Description
General anesthesia is almost always used. Local anesthesia may be used on selected occasions with heavy sedation or in the unconscious patient. A transverse or curved skin crease incision in the lower neck is usually used. The fascia between the strap muscles is divided in the midline to expose the thyroid isthmus. The thyroid isthmus is exposed at the second tracheal ring. Curved artery clips are passed beneath the isthmus using gentle dissection to avoid bleeding and the isthmus is clamped either side of the midline to expose the trachea. A square section of the anterior trachea is removed or a flap is created and brought outwards, hinged inferiorly. Good coordination with the anesthetist is important to withdraw the endotracheal tube before entry into the trachea. Care needs to be taken to avoid damage to the endotracheal tube or deflation of the cuff. Hemostasis is ensured using diathermy or occasionally ligatures if needed. Care should be taken to avoid ignition of gases or alcohol from diathermy, where used. A cuffed tracheal tube is inserted.
Anatomical Points
The anatomy of the neck is relatively constant in nature, but significant variations can occur with the shape and length of the neck (for example, short thicker “bull necked” individuals), which may impede access and to some degree alter the risk of complications. Large vessels may cross the neck, especially anterior neck veins and should be identified and ligated. Thyroid enlargement especially of the isthmus, although relatively rare, may also impede access to the trachea. Nerves are usually well away from the site of surgery in the midline and therefore of little risk (Table 7.2).
Table 7.2
Open tracheostomy estimated frequency of complications, risks, and consequences
Complications, risks, and consequences | Estimated frequency |
|---|---|
Most significant/serious complications | |
Infection | 1–5 % |
Bleeding/hematoma formation | 1–5 % |
Vascular injury | 1–5 % |
External jugular vein branches | |
Neural injury | 1–5 % |
Recurrent laryngeal nerve (X) | |
Cervical plexusa | |
Thyroid injurya | 1–5 % |
Damage to endotracheal tube/cuff | 1–5 % |
Respiratory obstruction | |
Early or late | 1–5 % |
Rare significant/serious problems | |
Tracheal necrosis | 0.1–1 % |
Tracheal stenosis | 0.1–1 % |
Tracheomalacia | 0.1–1 % |
Tracheal rupture | <0.1 % |
Surgical emphysema (major) | 0.1–1 % |
Persistent or recurrent cyst/sinus/fistula | <0.1 % |
Less serious complications | |
Pain or tenderness (sore throat; sore neck—transient) | |
Acute (<4 weeks) | >80 % |
Chronic (>12 weeks) | 1–5 % |
Seroma formation (persistent) | 1–5 % |
Numbness/altered sensation | 1–5 % |
Bruising | 50–80 % |
Dimpling/deformity of the skin | 1–5 % |
Dehiscence | <0.1 % |
Flap (skin) necrosis (significant) | 0.1–1 % |
Wound scarring (poor cosmetic result)a | 1–5 % |
Drain tube(s) | 5–20 % |
Perspective
The major risk and debility resulting from open tracheostomy surgery is bleeding. This may occasionally lead to a hematoma formation, rarely large enough to require surgical evacuation and hemostasis. Numbness of the neck is uncommon, but can be annoying, making shaving difficult causing injury, or making application of cosmetics difficult. Dehiscence and flap necrosis are often very minor and heal spontaneously or with limited dressings. Skin grafts or flaps are rarely required. Infection can rarely be significant. Respiratory obstruction is a potential problem (1) at entry to the trachea as the tracheostomy tube is inserted as the endotracheal tube is withdrawn, (2) later if the endotracheal tube dislodges and/or the tracheal flap (if used) obstructs the trachea, (3) at the time of tube changes, or (4) from blood clot or mucus plug obstruction. Excessive cuff pressure may lead to ulceration and tracheal necrosis. Tracheomalacia may lead to decreased rigidity of the cartilage in the trachea and tracheal collapse. Tracheal stenosis may result from fibrosis/scarring of the tracheal wall. Cosmetic deformity at the tracheostomy site in the central lower neck is common.
Major Complications
The most serious complications can arise from tracheal tube dislodgement causing respiratory obstruction, or damage to the trachea. Oxygen desaturation at the time of tracheostomy tube insertion can be a major issue if the airway is not maintained. Pre-oxgenation prior to tube insertion/manipulation is helpful in providing more safety and time. Bleeding may be significant and reduce vision and difficulty with placement of the tube into the trachea. Infection is rarely severe, but chronic purulent discharge around the tracheostomy tube entry site is not uncommon. Abscess formation and systemic sepsis are very rare. Surgical emphysema is rarely severe and due to air-leak around the tube into the tissues. Tracheal ulceration and necrosis may arise from excessive cuff pressure and prolonged tracheostomy or prior endotracheal intubation. Tracheal rupture is very rare. Tracheal stenosis may arise from fibrosis and scarring resulting from tracheal ulceration or necrosis. Cosmetic deformity from the indrawn scar is not uncommon, but needs to be balanced against the necessity for a tracheostomy.
Consent and Risk Reduction
Main Points to Explain
GA risk
Respiratory obstruction
Bleeding/hematoma
Wound infection
Abscess formation
Cosmetic deformity
Further surgery
Salivary Gland Surgery: Parotid Gland Surgery—Superficial Parotidectomy
Description
General anesthesia is almost always used, and no muscle relaxant, or a shorter acting one is preferred, to permit nerve stimulation. Superficial parotidectomy is removal of the superficial part (lobe) of the parotid gland. An incision is usually made just anteriorly to the ear extending into the upper neck. A pre-tragal lesion within the posterior portion of the gland may utilize a pre-tragal incision alone, allowing facial nerve dissection and tumor excision through a small incision. Lesions which are between the tragus and the angle of the jaw may be removed using a modified “S” incision around the lower ear and onto the neck, again with facial nerve dissection and tumor excision through a relatively small incision. The fine marginal mandibular branch of the facial nerve is usually avoided by keeping the incision at least 2 cm below the mandibular margin. The thin skin overlying the parotid gland is dissected and the flap is raised free from the gland. This procedure aims to dissect the parotid gland with preservation of the facial (VII cranial) nerve. The parotid duct branches are intentionally transected during the procedure, branches to the deeper parts of the gland usually remain. Dissection of the skin flap should be between the submuscular aponeurosis and the dermal layer to avoid risk of skin puncture and tumor capsule entry and allows good healing of the flap with excellent cosmetic outcomes. Nerve integrity monitoring can help in training surgeons in parotidectomy and to protect the nerve during dissection to avoid traction, which causes neuropraxia. A nerve stimulator can also confirm preservation of the nerve branches and likely recovery of any neuropraxia. Identification of the main VII nerve trunk arising from the base of the bony auditory canal at the angle with the mastoid, or tracing it back from a branch (an easy anatomical site to find a branch is over the retromandibular vein). Although all accidental injury should ideally be avoided, injury to the branch to orbicularis oculi branch is generally more debilitating than lower branch injuries. The gland is very vascular and oozing of blood is common, together with some salivary fluid leakage. For this reason, a wound drain is often used at completion (Figs. 7.1 and 7.2).

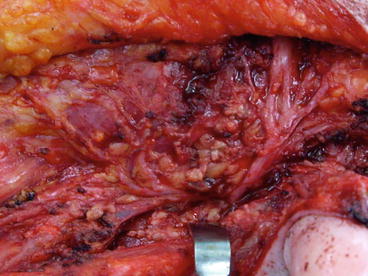
Fig. 7.1
Malignant parotid mass (melanoma) and facial (VII) nerve palsy
Fig. 7.2
Facial nerve (VII) exposed during a superficial parotidectomy
Anatomical Points
Variations in the course facial (VII) nerve are common with variable branching being typical between patients. Careful dissection following the facial nerve branches is usually performed either commencing from the main VII nerve trunk or with the fine branches backwards. A nerve stimulator is sometimes helpful in locating the facial nerve branches, as is the avoidance of long-acting paralyzing agents during anesthesia. Most of the variants of the mandibular branch of the VIIn. course lie within 2 cm of the inferior border of mandible, so that placement of incisions below this level reduces risk of injury. Injury to this branch causes drooping of the mouth on the same side. The zygomatic branch is usually small and can be tortuous. This branch supplies the orbicularis occuli m. and injury causes difficulty with eye closure. The VIIn. main trunk is usually relatively constant in position and found just deep to the bony prominence at the joint with the cartilaginous portion of the external auditory tube. Some neuropraxia of the VIIn. is usual due to the trauma of dissection (Table 7.3).
Table 7.3
Superficial parotidectomy estimated frequency of complications, risks, and consequences
Complications, risks, and consequences | Estimated frequency | |
|---|---|---|
Most significant/serious complications | ||
Infection | 1–5 % | |
Bleeding/hematoma formation | 1–5 % | |
Salivary collection/seroma formation (persistent) | 5–20 % | |
Facial nerve injury | − Overall (all) | 20–50 % |
− Permanent major | 0.1–1 % | |
− Permanent minor | 1–5 % | |
− Transient | 20–50 % | |
Auriculotemporal syndrome of Frey | ||
Frey’s syndrome (auriculotemporal nerve, facial nerve crossover causing gustatory sweating) | 20–50 % | |
Great auricular nerve injury (Earlobe numbness)a | 50–80 % | |
Tumor recurrence (benign or malignant)b | 1–5 % | |
Recurrent parotitisb | 1–5 % | |
Cyst recurrenceb | 1–5 % | |
First bite syndrome | 5–20 % | |
Rare significant/serious problems | ||
Salivary fistula | 0.1–1 % | |
Flap (skin) necrosis (significant) | 0.1–1 % | |
Sympathetic nerve/chain injury (rare) (Horner’s syndrome) | <0.1 % | |
Less serious complications | ||
Pain or tenderness (sore throat; sore neck—transient) | ||
Acute (<4 weeks) | 20–50 % | |
Chronic (>12 weeks) | 0.1–1 % | |
Bruising | 50–80 % | |
Numbness/altered sensation | 50–80 % | |
Twitching (facial muscles) | 5–20 % | |
Requirement for skin flaps or graftsb | <0.1 % | |
Dehiscence | <0.1 % | |
Wound scarring (poor cosmetic result)b | 1–5 % | |
Dimpling/deformity of the skin | 1–5 % | |
Drain tube(s)b | 1–5 % | |
Perspective
The major debility resulting from superficial parotidectomy is severe, permanent facial nerve injury resulting in ipsilateral complete facial paralysis. Minor injury to the facial nerve is not uncommon resulting in partial paralysis and facial drooping. Often, this affects one or two branches of the facial nerve and only the muscles supplied by these neural branches are then paralyzed. Minor paralysis or weakness is common and this usually will recover several weeks postoperatively. Residual weakness can be accompanied by twitching of some groups of the facial muscles; however, twitching can continue after recovery of sensory and motor function. Bleeding is usually minor, occasionally leading to a hematoma and rarely large enough to require surgical evacuation and hemostasis. The true frequency of nerve injuries, Frey’s syndrome, earlobe numbness, and twitching is difficult to accurately ascertain, since many patients will report a very mild form of these features. When closely examined and questioned, patients will often report short-lived symptoms especially when tired, stressed, or exposed to cold. Frey’s syndrome is rare prior to 6 weeks postoperatively and often stops spontaneously by 3–6 months, but topical antiperspirants or subdermal Botox may reduce symptoms of gustatory sweating. Numbness of the earlobe and of the face or neck is common and can be annoying, making shaving difficult causing injury, or making application of cosmetics difficult. First bite syndrome is pain on the initial bite each time when eating, which reduces with each subsequent bite. The true frequency of seromas, salivary collections, and even fistulae is uncertain since many are not reported or transitory (day to weeks) and are not considered significant. If prolonged, these may respond to botox injected into the residual gland. This poses almost no risk to facial nerve function. Dehiscence and flap necrosis are often very minor and heal spontaneously or with limited dressings. Skin grafts or flaps are rarely required. Longer-term complications of parotid gland surgery evolve over time. Recurrence of tumor or inflammation depends on the individual problem and situation. Tumor recurrence is maximal in the first 2 years after surgery, but can occur years after surgery. Wound infections usually occur as an early complication, within the first 3 days.
Major Complications
One of the most serious potential complications are total or partial facial nerve damage where all or some branches of the nerve may be affected, which in its most serious form leads to complete paralysis of the facial muscles causing lateral lip drooping, producing drooling, and difficulty closing the eye on the affected side causing occular trauma, keratitis, and corneal ulceration. This can be permanent, but usually partially or completely recovers, depending on the extent of injury. Further surgery may be required to promote eye and mouth closure. Frey’s syndrome (gustatory sweating) can occasionally be very severe producing excessive sweating with the smell or taste of food and very rarely requires surgical division of the auriculotemporal nerve. When tumor recurrence occurs after superficial parotidectomy for a pleomorphic adenoma or malignant tumor, it is typically in the form of multiple cutaneous/subcutaneous nodules. These can usually be excised with or without adjuvant radiotherapy. Radiotherapy or chemotherapy may be recommended for some malignant tumors treated by superficial parotidectomy. Seroma (or salivary collection) formation is not uncommon, but usually presents few problems for the patient in the long-term. Salivary fistula is rare and often closes spontaneously, but can be a significant problem if it fails to do so and becomes persistent. Recurrent parotitis can be a severe problem following superficial parotidectomy for intractable parotid inflammation. Severe skin flap necrosis is very rare because of the excellent vascular supply to the face, but necrosis may rarely require flap repair or free skin grafting. Horner’s syndrome, although very rare, can cause embarrassment for the patient due to the constricted pupil on the affected side. Numbness over the face and/or neck may be unpleasant and make shaving or cosmetic application problematic.
Consent and Risk Reduction
Main Points to Explain
GA risk
Respiratory obstruction
Bleeding/hematoma
Wound infection
Abscess formation
Cosmetic deformity
Further surgery
Salivary Gland Surgery: Parotid Gland Surgery—Total Parotidectomy
Description
General anesthesia is almost always used, and no muscle relaxant, or a shorter acting one is preferred, to permit nerve stimulation. Total parotidectomy is removal of the entire parotid gland including the superficial and the deep parts (lobes). Total parotidectomy is infrequently performed, usually for tumor resection. A modified “S” incision made just anteriorly and around the lower ear and onto the neck may be used. The facial (VII cranial) nerve may need to be sacrificed if involved with tumor and unable to be retained. The fine marginal mandibular branch of the facial nerve is usually avoided by keeping the incision at least 2 cm below the mandibular margin. The thin skin overlying the parotid gland is dissected and the flap is raised free from the gland. Dissection of the skin flap should be between the submuscular aponeurosis and the dermal layer to avoid risk of skin puncture and tumor capsule entry and allows good healing of the flap with excellent cosmetic outcomes. Nerve integrity monitoring can help in training surgeons in parotidectomy and to protect the nerve during dissection to avoid traction, which causes neuropraxia. A nerve stimulator can also confirm preservation of the nerve branches and likely recovery of any neuropraxia. Identification of the main VII nerve trunk arising from the base of the bony auditory canal at the angle with the mastoid, or tracing it back from a branch (an easy anatomical site to find a branch is over the retromandibular vein). Although all accidental injury should be ideally avoided, injury to the branch to orbicularis oculi branch is generally more debilitating than lower branch injuries. The parotid duct is transected and usually ligated during the procedure. The gland is very vascular and oozing of blood is common. A wound drain is often used at completion. Malignant involvement of the nerve will necessitate sacrifice of involved branches or the entire nerve.
Anatomical Points
Total unilateral facial muscle paralysis occurs if the facial nerve is divided and resected. The smaller, deep part of the parotid gland extends posterior to the ramus of mandible effectively between the external and internal carotid arteries. Variations in the course facial nerve are common with variable branching being typical between patients. If retained, careful dissection following the facial nerve branches is usually performed either commencing from the main VII nerve trunk or sometimes with the fine branches backwards. A nerve stimulator is sometimes helpful in locating the facial nerve branches, as is the avoidance of long-acting paralyzing agents during anesthesia. Most of the variants of the mandibular branch of the VIIn. course lie within 2 cm of the inferior border of mandible, so that placement of incisions below this level reduces risk of injury. Injury to this branch causes drooping of the mouth on the same side. The zygomatic branch is usually small and can be tortuous. This branch supplies the orbicularis occuli m. and injury causes difficulty with eye closure. The VIIn. main trunk is usually relatively constant in position and found just deep to the bony prominence at the joint with the cartilaginous portion of the external auditory tube. Some neuropraxia of the VIIn. is usual due to the trauma of dissection (Table 7.4).
Table 7.4
Total parotidectomy estimated frequency of complications, risks, and consequences
Complications, risks, and consequences | Estimated frequency | |
|---|---|---|
Most significant/serious complications | ||
Infection | 1–5 % | |
Bleeding/hematoma formation | 1–5 % | |
Salivary collection/seroma formation (persistent) | 5–20 % | |
Facial nerve injury | − Overall (all)a—if preserved | 20–50 % |
− Permanent majora | 1–5 % | |
− Permanent minor | 5–20 % | |
− Transient | 20–50 % | |
− Complete paralysis—if sacrificeda | 100 % | |
Auriculotemporal syndrome of Frey | ||
Frey’s syndrome (auriculotemporal nerve, facial nerve crossover causing gustatory sweating) | 20–50 % | |
Great auricular nerve injury (Earlobe numbness)a | 50–80 % | |
Cervical plexus injurya | 5–20 % | |
Tumor recurrence (benign or malignant)a | 1–5 % | |
Recurrent parotitisa | 1–5 % | |
First bite syndrome | 5–20 % | |
Rare significant/serious problems | ||
Salivary fistula | 0.1–1 % | |
Flap (skin) necrosis (significant) | 0.1–1 % | |
Sympathetic nerve/chain injury (rare) (Horner’s syndrome) | <0.1 % | |
Less serious complications | ||
Pain or tenderness (sore throat; sore neck—transient) | ||
Acute (<4 weeks) | 20–50 % | |
Chronic (>12 weeks) | 0.1–1 % | |
Bruising | 50–80 % | |
Numbness/altered sensation | 50–80 % | |
Twitching (facial muscles) | 5–20 % | |
Requirement for skin flaps or graftsa | <0.1 % | |
Dehiscence | <0.1 % | |
Wound scarring (poor cosmetic result)a | 1–5 % | |
Dimpling/deformity of the skin | 1–5 % | |
Drain tube(s)a | 1–5 % | |
Perspective
The major debility potentially resulting from total parotidectomy is severe, permanent facial nerve injury resulting in complete ipsilateral facial paralysis. If the nerve is infiltrated with tumor, then the nerve may require to be sacrificed. Minor injury to the facial nerve is not uncommon if the nerve is preserved, often arising from extensive dissection, resulting in partial paralysis and facial drooping. This may affect one or more branches of the facial nerve and only the muscles supplied by these neural branches are then paralyzed. Minor paralysis or weakness may recover several weeks postoperatively. Residual weakness can be accompanied by twitching of some groups of the facial muscles; however, twitching can continue after recovery of sensory and motor function. Because dissection for total parotidectomy is often greater than for superficial parotidectomy the relative risk of facial nerve injury is higher. Bleeding is usually minor, occasionally leading to a hematoma and rarely large enough to require surgical evacuation and hemostasis. The true frequency of nerve injuries, Frey’s syndrome, earlobe numbness, and twitching is difficult to accurately ascertain, since patients will report a very mild form of these features. When closely examined and questioned, patients will often report short-lived symptoms especially when tired, stressed, or exposed to cold. Frey’s syndrome is rare prior to 6 weeks postoperatively and often stops spontaneously by 3–6 months, but topical antiperspirants or subdermal Botox may reduce symptoms of gustatory sweating. First bite syndrome is pain on the initial bite each time when eating and reducing with subsequent bites. Numbness of the earlobe and of the face or neck is common and can be annoying, making shaving difficult causing injury, or making application of cosmetics difficult. First bite syndrome is pain on the initial bite each time when eating and reducing with subsequent bites. The true frequency of seromas, salivary collections, and even fistulae is uncertain since many are not reported or transitory (day to weeks) and are not considered significant. If prolonged, these may respond to botox injected into the residual gland. This poses almost no risk to facial nerve function. Dehiscence and flap necrosis are often very minor and heal spontaneously or with limited dressings. Skin grafts or flaps are rarely required. Longer-term complications of parotid gland surgery evolve over time. Recurrence of tumor or inflammation depends on the individual problem and situation. Tumor recurrence is maximal in the first 2 years after surgery, but can occur years after surgery. Wound infections usually occur as an early complication, within the first 3 days.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


