POPULATION
Hearing impairment is one of the most prevalent chronic disabilities in the United States. Approximately 34.25 million Americans have hearing impairments (
1). The prevalence of hearing loss nearly doubled from 1965 to 1994, and the growth is predicted to continue (
2). In the aging population, hearing loss is prevalent in nearly two-thirds of those over the age of 70 in the United States (
3); these estimates are even higher in those with cognitive impairment such as dementia (
4). Risk factors for hearing loss trend toward poor socioeconomic status, men more than women, and whites more than any other ethnicity (
5). Hearing loss is associated with increased isolation (
6) and functional and cognitive decline (
6,
7).
Hearing loss is most common in the aging population but also affects children; nearly 8% of those with permanent hearing loss are children (
8). On any given day, 43% of elementary school students have a mild hearing loss (
9). Congenital hearing loss affects 1 to 6 per 1,000 newborns (
10). Most children with congenital hearing loss will be affected at birth and can potentially be identified by newborn hearing screening; however, some hearing losses may not be evident until later in childhood (
11). Recent evidence suggests that hearing impairment in the teenage population is on the rise (
12). The consequences of hearing impairment in both children and adults are detrimental to social involvement. Poor hearing leads to communication impairments and progressive social isolation that may impact overall health (
13,
14). Many of the health and social consequences of hearing loss can be mitigated with a comprehensive auditory (re)habilitation program of which hearing aids will be a part.
Individuals pursue hearing aids and assistive listening devices when there is no medical/surgical treatment that will resolve their hearing loss or if they are not candidates for medical/surgical intervention. For children, they may need an amplification system before they are old enough for specific surgical interventions that will later resolve conductive hearing loss. The encouraging news for individuals with permanent hearing loss is that there are treatments for all types and degrees of hearing loss at this time. The treatments will not restore normal hearing but should assist the individuals in their daily communication activities and provide a safe environment in which to function.
Pursuing amplification is a process that continues for the life of an individual. There is the initial process of selecting, fitting, and adjusting to the hearing aids and then the ongoing process of maintenance, replacement, and upgrade of the devices over time. Therefore, the patient establishes a relationship with the individual providing their amplification as part of a larger auditory (re)habilitation process. Otolaryngologists who may be managing the medical care of patients with hearing loss also will want to have a relationship with a professional they trust to take care of their patients’ amplification and auditory (re) habilitation needs. The audiologist plays this role for the patient and otolaryngologist and is educated in the area of hearing assessment and hearing aid selection and fitting. The patient is provided with complete hearing health care when in the care of both the otolaryngologist and audiologist who are coordinating their services.
GOAL OF AMPLIFICATION
The reduction in hearing sensitivity produced by hearing loss results in activity limitations and participation restrictions as defined by the World Health Organization’s International Classification of Functioning, Disability, and Health (
15). Solutions to these challenges will come in the form of a comprehensive auditory (re)habilitation program that will include counseling, communication training, environmental modifications, speech and language development for children, and amplification.
Amplification is only one part of a complete auditory (re) habilitation program and should be viewed in the context of a larger program.
The basic goals of a hearing aid fitting are to provide audibility for the range of sounds encountered in daily life (range of intensity levels and frequencies), to allow the listener to hear in complex (noisy) situations commonly occurring in daily communication, and to do all this while being comfortable acoustically and physically. With the advent of a variety of consumer electronics designed to couple to the ear, a newer challenge is making sure these devices couple to the hearing aid that is coupled to the ear. While maintaining comfort, the properly fit amplification system makes the world of sound accessible to the user.
BASICS OF THE AMPLIFICATION SYSTEM
A basic amplification system is depicted in
Figure 164.1. Every hearing aid functions in the manner described in
Figure 164.1 including an acoustic input signal to the microphone, an analog/digital (A/D) converter, an amplification stage, a digital/analog (D/A) converter, and then the electric signal being converted to an acoustic signal as it leaves the receiver (loudspeaker) and enters the ear canal. The amplification stage is contained within the digital chip and may include differential amplification at various frequencies (channels). In addition, amplification may be differentially applied to certain levels of input (e.g., soft, moderate, loud) and to certain types of inputs (noise, speech, music) based on the algorithm driving the hearing aid signal processing. These details are described later in the chapter.
HEARING AID FITTING PROTOCOLS
This chapter is meant to introduce the physician to the many options and decisions that must be made when assisting patients in the selection of the appropriate amplification system for their hearing loss, communication needs, and lifestyle. In addition, the best practice components of hearing aid verification and outcome assessment are highlighted. Since the physician may be the entry point into hearing health care, the material in this chapter should better prepare them to discuss possible amplification solutions with their patients and help prepare them for the process they will encounter in order to become a successful hearing aid user. For detailed, evidence-based guidelines for the selection, fitting, verification, and outcome assessment of amplification systems for pediatric patients, the reader is referred to the American Academy of Audiology (AAA) Pediatric Amplification Guidelines (
16). For evidence-based guidelines related to the provision of hearing aids in adults, the reader is referred to the AAA Guidelines for the Audiologic Management of Adult Hearing Impairment (
17).
HEARING LOSS AND CANDIDACY
The AAA Pediatric Amplification Guidelines (
16) indicate, “Amplification with hearing instruments should be considered for a child who demonstrates a significant hearing loss, including sensorineural, conductive, or mixed hearing losses of any degree.” (p. 2). Children are now being fit with hearing aids by the age of 6 months due to successful early identification programs and the new guidelines that suggest children should be screened for hearing loss by 1 month, diagnosed by 3 months, and fit within 1 month of diagnosis and no later than 6 months (1-3(+1)-6 goal) (
18). The AAA Guideline for the Audiologic Management of Adult Hearing Impairment (
17) does not specifically outline candidacy but indicates that adult amplification recommendations will be based on the hearing evaluation and the patient’s reported difficulties. If an adult is having problems hearing, then he or she is a candidate for hearing assistance. A recent study (
19) found that the question “On a scale from 1 to 10, 1 being the worst and 10 being the best, how would you rate your overall hearing ability?” could sort out which individuals were ready to pursue amplification (1 to 4 rating), which individuals needed more counseling (5 to 7), and which individuals were not ready to pursue amplification (8 to 10).
EVALUATION
Physical examination of the auricle, external auditory canal, tympanic membrane, and middle ear space should be conducted. It is important to recognize conditions that warrant medical or surgical intervention or findings that would preclude tolerance of a device in or over the ear. A comprehensive audiogram that includes ear-specific pure-tone air- and bone-conduction thresholds, speech reception threshold, and word recognition testing is often the starting point of the hearing aid discussion. This level of detail will not be available for an infant, and yet our goal is to fit an infant with significant hearing loss with amplification within 1 month of diagnosis. For this purpose, ear-specific thresholds (via auditory brainstem response) in one low and one high frequency will suffice to
get the hearing aid fitting started. In the case of infants and young children, diagnostics are ongoing and the hearing aid fitting will be altered as more data related to the child’s hearing loss are gathered.
With the adult patient, there are other assessments that will assist in making recommendations related to specific hearing aid configurations and technology. The quantification of frequency-specific thresholds of discomfort has been found to improve the hearing aid fitting (
20). In essence, the individual’s dynamic range needs to be defined in order to appropriately tune the hearing aid to produce outputs for soft, moderate, and loud sounds all within the audible but comfortable range for the individual. The lower boundary of the dynamic range is defined through threshold assessment. If thresholds of discomfort are not measured individually, then we are allowing the upper boundary of the individual’s dynamic range to be defined as an average for the population. Measures of uncomfortable loudness are simple to perform and add to the precision of the hearing aid fitting. If these measures are not accomplished prior to the fitting, the clinician must be sure to verify that the individual’s tolerance level has not been exceeded by use of average data through a verification procedure prior to the individual leaving the clinic.
An assessment of the individual’s speech comprehension in noise also may be considered prior to recommending various amplification features. Two commonly used speech in noise tests include the Hearing in Noise Test (
21) and the QuickSIN (
22). A signal-to-noise ratio value is determined from these tests and can be compared to the performance of normal listeners. The QuickSIN provides ranges that relate to technology recommendations (e.g., use of directional microphones, use of assistive listening devices). In addition, the results can be very helpful in counseling the patient about realistic expectations when communicating in noise and potential environmental manipulations that may be necessary.
There is compelling evidence that if individuals want to hear in noise, they need to use two hearing aids if they have hearing loss in both ears (
23). With that said, there are individuals who have binaural interference meaning that sound coming into one ear is interfering with the processing of sound from another. A dichotic test requiring hearing from both ears in order to successfully complete the test can be used to identify individuals who may be better off with one hearing aid rather than two (
24). Some clinicians prefer to proceed with fitting two hearing aids allowing the individual to experience bilateral amplification and to compare that with wearing one hearing aid. This allows the hearing aid user to be part of the decision.
With these objective data in hand, the clinician will want to conduct an interview with the patient in order to assess current communication challenges, communication needs at home, in social situations, during hobbies or weekend activities, and in the workplace or school setting. In the case of a young child, the interview will be conducted with a parent or guardian. Older children should be engaged in this process. Answers to these questions may impact style, feature, and signal processing decisions as well as bring up the need for alternate solutions. For instance, if an individual is an avid bicyclist, then a style of hearing aid that can be worn comfortably with a bike helmet will be essential. In addition, the clinician may want to recommend special solutions to deal with moisture from rain and perspiration associated with this activity (see a list of special hearing aid solutions in
Table 164.1). There also are systematic questionnaires available to assist in this part of the assessment including the Abbreviated Profile of Hearing Aid Benefit (
25), Client Oriented Scale of Improvement (
26), and the Expectations Worksheet (
27). Identifying the patient’s current expectations of amplification can be very helpful for creating appropriate recommendations and for motivating a conversation about realistic expectations (e.g., amplification does not return normal hearing).
PRESELECTION DECISIONS
Once the clinician is knowledgeable about the individual’s hearing status, communication needs, and lifestyle, there are a variety of preselection decisions to be made. Currently, there are fewer decisions that have to be made prior to ordering the devices than in the past because many hearing aids now contain options to turn on or off various features (e.g., volume control, directionality), but some decisions continue to impact the device that will be ordered for the patient. These decisions are outlined below.
ROUTING OF THE SIGNAL
The signal from an amplification device can be delivered via air or bone conduction. In the case of a cochlear implant, the signal is electric. Cochlear implants are used by individuals with severe to profound hearing loss who do not receive benefit from traditional amplification. The needs of these patients and this technology are covered elsewhere in this text. There is evidence to encourage unilateral cochlear implant users to continue or start to use amplification on the non-implanted side (
28,
29). For the majority of patients with sensorineural hearing loss, an air conduction system will be recommended. Depending on the configuration of the hearing loss, various amplification arrangements may be pursued. The individual with bilateral hearing loss generally will benefit from amplification in both ears.
The individual with severe unilateral hearing loss (singlesided deafness or unaidable hearing on one side due to extremely poor clarity) may consider several recommendations that would include (a) continuing to rely on the good ear without amplification (this poses problems whenever the individual is trying to listen to someone on his/her “bad” side), (b) using a CROS (contralateral routing of signal) system where a microphone is placed on the “bad” ear and
the signal is transferred (FM transmission) to a device that delivers the sound to the good ear, (c) a bone conduction hearing aid or device on the “bad” side that picks up sound from that side and delivers it to the “good” cochlea via bone transmission, and (d) a transcranial CROS that works in the same manner as the bone conduction aid but provides such an intense air conduction signal in the “bad” ear that the sound crosses over to the “good” cochlea via bone conduction. If the individual has some hearing loss in the “good” ear as well, a bilateral CROS (BICROS) system that not only provides a transfer of the signal from the “bad” ear but also provides amplification to the “good” ear can be used.
In the case of the bone conduction solution, this can be achieved through a bone vibrator coupled to the head on a tight band or through a bone vibrator attached to the skull with a titanium screw. There are two devices on the market currently used for this surgical solution. Both function in a similar manner. An implanted bone conduction hearing device is a type of hearing aid that transmits sound to the inner ear via bone conduction. It is appropriate to use in cases of conductive hearing loss, mixed hearing loss, or single-sided deafness. It also may be used for patients with hearing loss who cannot wear an air conduction hearing aid due to malformations or pathologies of the outer and/or middle ear. After the patient has been identified as a candidate based on the audiologic and medical examinations, a titanium screw is surgically implanted into the mastoid region of the temporal bone. The external portion of the screw, typically referred to as the abutment, is used to anchor the bone conduction unit to the head. The titanium fixture must become osseointegrated before the bone conduction unit can be affixed. The processor converts incoming sound to vibrations that stimulate the cochlea. Another option more recently available provides an abutment free option by using an implanted magnet to affix the external sound processor to the titanium implant. This is covered in greater detail in Chapter 163.
Another device based on bone conduction transmission is attached to maxillary teeth through a dental appliance that is removable. Sound is picked up by a microphone processor, and the signal is wirelessly delivered to the oral appliance. This device also is indicated for conductive or mixed hearing loss and single-sided deafness.
The individual with conductive hearing loss who does not wish to or cannot have medical/surgical intervention may pursue amplification. An air conduction hearing aid
can be used for mild-to-moderate conductive losses that are not accompanied by malformation of the outer ear or drainage. For conductive losses that are accompanied by malformations of the pinna and ear canal or that produce ongoing drainage, a bone conduction amplifier will be a better choice. In the case of pediatric patients, they may have a time period when they are waiting for their system to mature enough for surgical intervention (reconstruction) and will need to use a bone conduction hearing aid in order to keep the cochlea stimulated during this waiting period. As described above for solutions to single-sided deafness, a bone vibrator on a tight headband or an implanted bone vibrator can be used for this purpose. Currently, the FDA does not allow implantable bone vibrators for children under 5 years of age.
STYLE
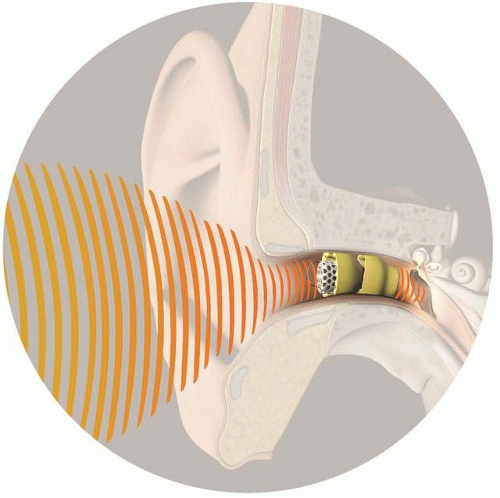
For patients receiving air conduction amplification, the discussion of the style of the hearing aid will be driven by the patient’s hearing loss, communication needs, lifestyle, and personal preferences. The discussion will start with defining whether the individual is interested in an extended wear option or a traditional wear option. Currently, there is one extended wear product commercially available, the Lyric hearing aid (
Fig. 164.2). This hearing aid is a single-channel, analog device that is disposable. Because of this level of technology, the battery life for this hearing aid is drastically increased. The Lyric is placed deep within the ear canal by the clinician after setting the programming based on coupler measurements (a probe microphone cannot fit in the ear canal when the device is inserted). The user has a magnet that allows them some control over the volume of the device. The Lyric provides 24/7 hearing with the user being able to shower and carry on most daily activities with the device in place. When the device stops working (this could range from a few weeks to 3 months depending on moisture, cerumen, etc.), the user has a tool that allows removal. The patient subsequently returns to the clinic or office for placement of a new device. To be a successful extended wear user, the individual needs to have reasonably cylindrical, straight ear canals. The manufacturer provides a systematic way to determine candidacy, sizing, and placement. The pricing structure of this device currently is quite different from traditional wear hearing aids and includes paying a yearly subscription fee.
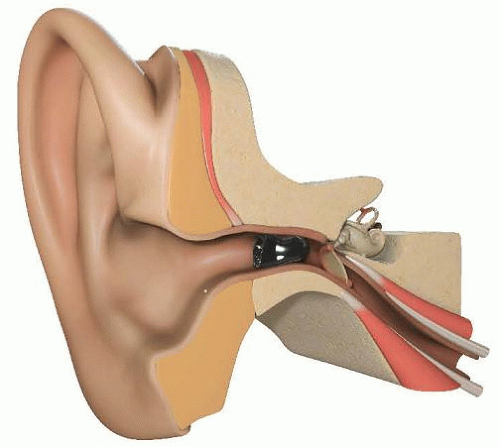
Recently, several manufacturers have introduced a deep insertion traditional wear hearing aid. This provides the benefit of the sound source being right near the tympanic membrane, which provides a wider, audible high-frequency bandwidth. However, this hearing aid is removed each night and batteries are replaced when they stop functioning (as opposed to the hearing aid being disposable). A picture of the new “invisible in canal (IIC)” hearing aid is provided in
Figure 164.3.
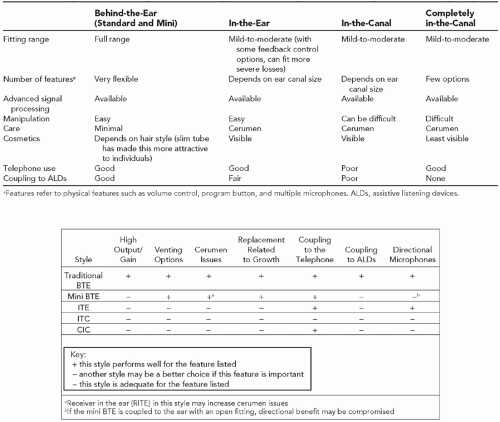
Individuals interested in traditional wear hearing aids have several styles and coupling options (connecting the hearing aid to the ear) to consider.
Figure 164.4 provides pictures of the various styles of hearing aids currently available along with a list of pros and cons.
Figure 164.5 provides the same type of information but focused on the pediatric patient whose outer ear will be growing over the first years of life. For pediatric patients, the behind-the-ear style is recommended because this style reduces the cost of refitting (only the earmold that couples the hearing aid to the ear needs to be replaced when the outer ear grows), provides the greatest amount of flexibility in terms of power (in case the hearing changes), offers a variety of features (ability to connect to assistive listening devices, etc.), and requires the least amount of maintenance. The final decision on style will be a balance of the clinician’s recommendation and the patient’s preferences.
Some of the most important changes in style recently have included the extended wear option, deep insertion
completely in the canal (CIC), and ability to provide more gain in a CIC with advances in feedback management, which has allowed more users to pursue this style without operating at the limits of amplification. In addition, the behind-the-ear (BTE) hearing aid has become a popular option with adults due to miniaturization (see a mini BTE in
Fig. 164.4) and the use of slim tube rather than standard tubing to couple the aid to the ear canal. In addition, with the advent of improved feedback management systems, open fit BTEs (
Fig. 164.6, panel B) that leave the ear canal much more open than traditional earmolds (
Fig. 164.6, panel A) have improved comfort and fit for many individuals. There has been some confusion in terminology with clinicians referring to any BTE with a slim tube as an “open fitting.” The slim tube can be connected to a dome allowing for an open fit, but it also can be connected to a standard earmold producing a closed fit for individuals who have more significant hearing loss.
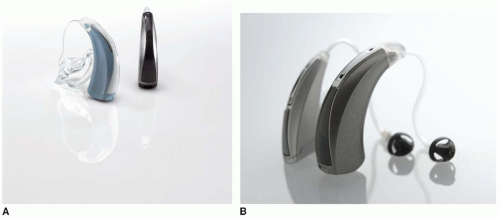
Figure 164.7 provides the various coupling arrangements that currently are available for BTE fittings. With the goal of slimming down the BTE but maintaining a reasonable battery life (1 to 2 weeks), manufacturers have introduced the receiver in the canal (RIC) BTE. The RIC is compared to a receiver in the aid (RITA) in
Figure 164.8 (RIC on the left and RITA on the right). An electrical connection from the BTE to the receiver housed inside the dome (or earmold) can be seen. By moving the receiver into the ear canal, the BTE case can be smaller while also holding a larger battery. The consequence, however, is cerumen damage to the RIC, whereas when the receiver is cased in the BTE, it is removed from potential cerumen damage. Because of this and the desire to make the CICs have a deeper insertion yet remain more dependable, cerumen guards (
Fig. 164.9) are a standard on all hearing aids with receivers in the canal.