37 Hearing Aids
Hearing aids are probably the fastest changing technology in the field of communication disorders. However, there are basic principles that apply to the selection and fitting of the devices that remain relatively stable as the hardware and software change regularly. The purpose of this chapter is to review those principles and provide descriptions of those components that are likely to change so that the reader can be cognizant of the areas that will require further exploration with individual manufacturers to remain current. The process begins with a thorough determination of the need for amplification. As the candidacy is determined, the need for appropriate features for successful use may be assessed. Next, the array of options must be considered and the appropriate device selected. During the fitting process, the goal is to provide beneficial amplification through accurate setting of the hearing aid features based on the audiometric and case history information. However, the fitting is not complete until it is confirmed that the intended benefits are received, that is, the fitting is validated. Furthermore, all hearing aids have limitations and will provide the greatest benefit when combined with other assistive listening technology to maximize communication. Most importantly, however, would be for the hearing aid to be dispensed/sold as part of a comprehensive auditory rehabilitation program. Even an individual with the most advanced digital amplification circuitry may experience failure when family members expect conversation from a distant room with no visual cues. Therefore, auditory rehabilitation should be offered with every hearing aid purchase so that individuals can learn the behavioral techniques that will lead to successful hearing aid use.
Hearing Aid Candidacy
Anyone with reduced hearing capabilities is a potential candidate for amplification. However, several other factors must be considered to determine if, in fact, they are a candidate. These factors can guide the astute audiologist into the next stage, hearing aid selection, because the information gathered to determine candidacy also provides clues to the possible style, features, and programs that may benefit an individual. There are three main areas to consider in determining candidacy: audibility, daily listening experiences, and handicap assessment. The information gathered from these assessments can be used to guide the audiologist to more efficiently select and fit the amplification and determine the appropriate rehabilitation program. The objective is to avoid trying amplification styles or features that might be rejected by the user because of difficulty with controls or lack of need for advanced features. In many cases, this information is just as important to overall success as is the actual gain and output settings. Therefore, an amplification candidacy form was developed as shown in Fig. 37.1 to document the critical information to be considered in the subsequent step, amplification selection.
Three aspects of audition potentially impact candidacy for amplification. These are degree, configuration, and type of hearing loss. For mild hearing losses, the need for amplification may be questionable and may be strongly influenced by the daily listening challenges and the results of the handicap assessment. For severe-to-profound losses, amplification can provide benefit even if it is simply sound awareness. Because average conversational speech is approximately 50 dB hearing loss, persons with hearing loss at or greater than that will hear only the intense vowel segments in speech and have a moderate need for amplification to restore much of the audibility of the consonant sounds. Another factor that might impact this is the slope of the hearing loss. The more similar the thresholds are across frequencies, that is, flat configuration, the more likely that the audibility for speech may be restored. Someone with a steeply sloping loss will likely have more difficulty adjusting to the restored high-frequency information that has been missing for possibly several years. Research has shown that the brain may reorganize following auditory deprivation such that areas of the cortex no longer respond to high-frequency information.1 When these high-frequency sounds are restored, the auditory areas of the brain can reorganize again to recognize these sounds again. Because this process may complicate the adjustment to amplification, the individual with steeply sloping hearing loss should be cautioned regarding expectations for immediate benefit. The type of hearing loss is important as it relates to inner ear damage. Persons with conductive hearing loss will typically be more successful users than those with sensorineural or mixed hearing loss because they are experiencing primarily a reduction in absolute sensitivity which can be more easily addressed via amplification than the effects of cochlear damage.
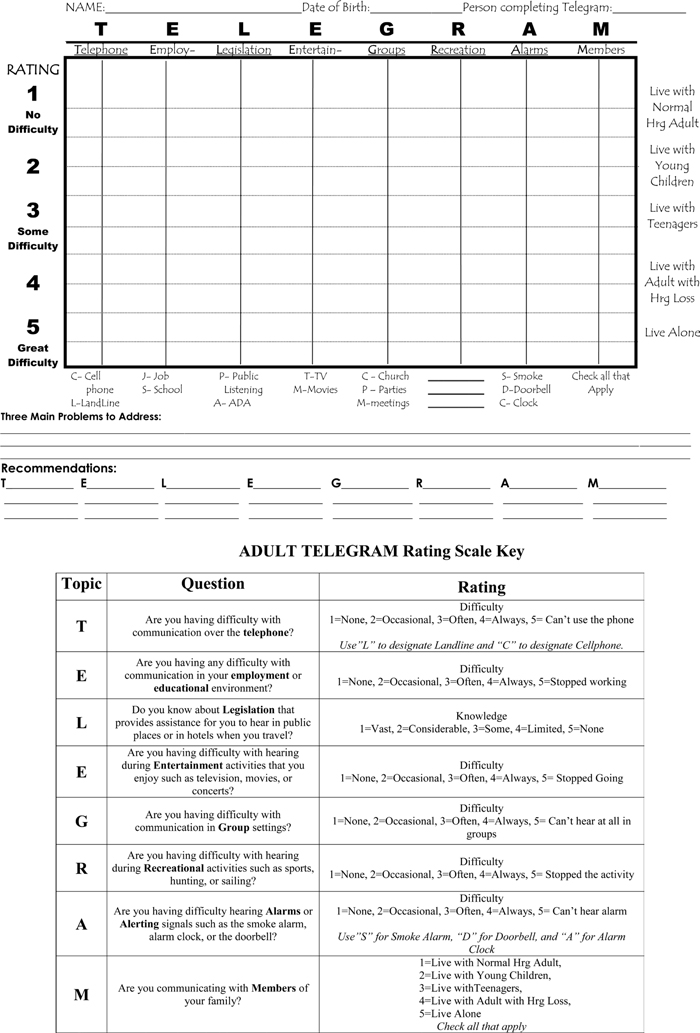
In addition to considering auditory sensitivity, the individual’s communication difficulties on a daily basis must be considered relative to candidacy. Although the Telephone, Education, Legislation, Entertainment, Groups, Recreation, Alarms, Members of House (TELEGRAM) was originally designed as a rehabilitation assessment tool,2 it also can be used to evaluate the candidacy for amplification with respect to daily listening experiences. Each letter represents an area that should be investigated with every individual who seeks an audiological evaluation. As shown in Fig. 37.2, each area is given a rating that reflects the degree of difficulty in that area. The more difficulty one experiences with hearing on the telephone, in employment settings, in groups, during recreation, and/or alarm signals the higher the rating. Difficulty in these areas may lead to selection of certain features on the hearing aid. For example, someone with difficulty hearing on the phone and manual dexterity problems might be a candidate for an auto T-coil feature. The sum of the ratings can be recorded on the candidacy form to illustrate the general need for amplification.
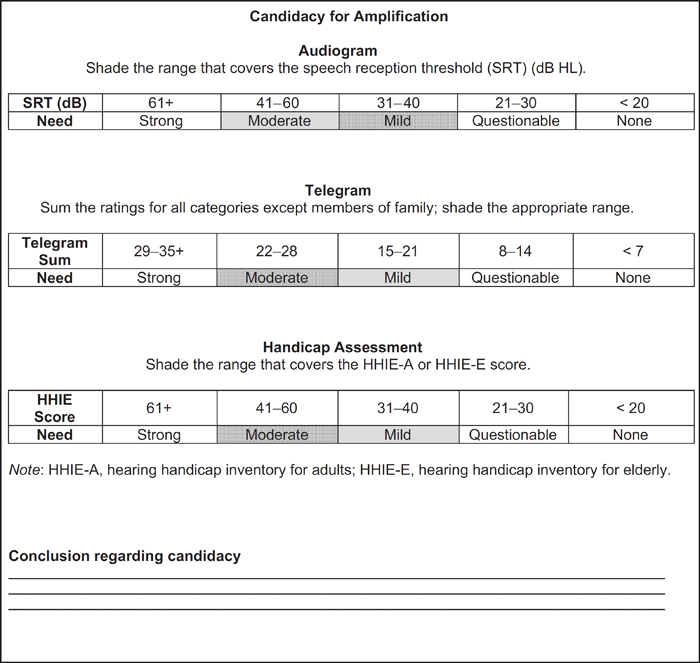
Figure 37.1 Three areas to assess to determine candidacy for amplification. Example of determining candidacy for amplification using the three criterion areas. The solid shaded areas represent someone with a moderate hearing loss and the striped areas represent someone with a mild degree loss but very different communication demands and reactions to the communication challenges.
The final major area to consider in determining hearing aid candidacy is the individual’s own assessment of his/her communication challenges. Some of this information may be determined while taking the case history when questions are posed about why they are seeking an audiological evaluation. However, a more objective tool is the hearing handicap inventory for adults (HHIA)3 or the hearing handicap inventory for the elderly (HHIE).4 These are short questionnaires designed to explore the emotional and social consequences of hearing loss through questions that can be answered as “yes,” “sometimes,” or “no.” The answers are assigned 2, 1, or 0 points, respectively, which are summed to provide a total score. Weinstein, Spitzer, and Ventry5 evaluated an 80 year-old Veterans Affairs Audiology participants and reported an average total score of 57.4 on the HHIE and social and emotional scores of 25.5 and 29.1, respectively. By noting the total score on the candidacy form in Fig. 37.1, one can determine the estimated need for amplification. For example, the average score on the HHIE of 57.4 reported by Weinstein et al would fall in the area of “moderate need.”
Hearing Aid Selection
The task of selecting the most appropriate hearing aid involves considerations of not only the physical abilities of the individual but also his/her surroundings and associated communication demands. These considerations may be grouped into four major areas which include the style/coupling of the hearing aid, the features, the electroacoustic characteristics, and the manufacturer. Hearing aid consumers often have preconceived notions regarding the style of aid they prefer based on others they have seen. If they are experienced users they may even have a preference for a particular manufacturer stemming from their own previous experience. However, most consumers rely on the professional for guidance to the particular features and specific electroacoustic settings.
The various styles of hearing aids are shown in Fig. 37.3. The taxonomy that has been perpetuated over the years is based primarily on the location of the circuitry. Of particular importance is the location of the microphone. In the custom styles such as in-the-ear (ITE), in-the-canal (ITC), completely-in-the-canal (CIC), the microphone is in the pinna, opening of the ear canal, or actually in the ear canal which provides various degrees of beneficial resonance of high-frequency information. The other advantage of these styles is the natural reduction of noise from the rear created by the pinna. Another style that takes advantage of these factors that has been gaining popularity in the past 5 years is a disposable miniature hearing aid that is inserted deep into the ear canal shown in Fig. 37.4. Because it is not removed daily, it is also known as an extended-wear device. The microphone of this deeply-inserted hearing aid is as close to the natural reception of sound waves as possible so that the individual benefits from pinna, concha, and ear canal resonances. A variation of this microphone placement within the pinna area is shown in Fig. 37.5 where the custom shell is placed in the canal but the microphone is outside the shell and fits up in the helix. Aids that are worn over the pinna are traditionally called behind-the-ear (BTE) aids. Because the microphone is at the top, there is greater access to receive unwanted signals such as wind or noise from behind than with the custom aids.

Figure 37.3 Various styles of hearing aids.
Source: http://www.phonak.com/us/b2c/en/products/hearing_instruments/all_products.html.
Rather than the standard tubing leading to a custom earmold, many users prefer a very slim tube that has a flexible dome on the end for coupling to the ear. This saves considerable time in the fitting process by not having to take an earmold impression and wait for the custom mold. When a tip is selected with several large vents, it may be called an “open fit.” This is ideal for persons with minimal hearing loss in the low frequencies because the vents will allow the low-frequencies to escape out of the ear canal. The maximum achievable gain is less with the slim-tube fitting than with the standard custom earmold.
Another recently popular hearing aid style is known as the receiver-in-the-canal (RIC). Because the receiver component is removed from the hearing aid case and placed in the ear canal encased in a flexible dome tip, the portion worn on the ear is considerably smaller and therefore more cosmetically appealing. Furthermore, because the receiver is placed in the ear canal, less gain is required than when it is in the traditional position in the hearing aid case.
In the MarkeTrak reports of hearing aid satisfaction, the respondents who wore traditional styles including BTE, ITE, ITC, and CIC accounted for approximately 65% of sales over the period 2005 to 2008.6 A rise in the more innovative styles compared with previous years was reported. Another 25% of the sales were “mini-BTE” which included open-fit or slimtube fittings or the RIC, as well as the smaller aids fit with traditional tubing and earmolds also called on-the-ear (OTE) hearing aids. The final 10% of sales was the “invisible” aid which is placed deep in the canal for extended wear.
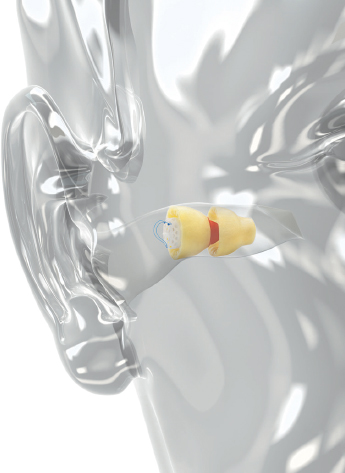
Figure 37.4 Extended wear hearing aid deeply inserted in the ear canal.
Source: http://www.lyrichearing.com/lyric-hearing-aid-news-events.
When determining the hearing aid style, the first question to consider is whether or not the individual has experience with amplification. If so, the success, or lack thereof, with the previous fitting should be explored as it relates to a possible change in style. For persons who are new to amplification, the degree of the hearing loss is the first consideration that may limit particular style options. For persons with mild-to-moderate hearing loss, any style of hearing aid could be selected. However, for more severe losses, the traditional BTE, full-shell ITE, and possibly a RIC with the receiver secured in a custom mold may be selected.
There are some special circumstances that result in a unique style of hearing aid. Persons with unilateral hearing loss are at a disadvantage in noisy environments and when the speech is coming from the side of their hearing loss. One solution is to fit a microphone on the poor ear that would pick up sound and send it to the good ear via a short-range FM arrangement. This Contralateral Routing of the Offside Signal (CROS) is housed in BTE cases so that the individual wears something on each ear typically coupled with open fitting earmolds. If the better ear also has some hearing loss, gain can be added to the BTE on that side and then it becomes a BI-CROS.
Another type of hearing aid that addresses this problem is known as a bone-anchored hearing device (BAHD). As show in Fig. 37.6
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


