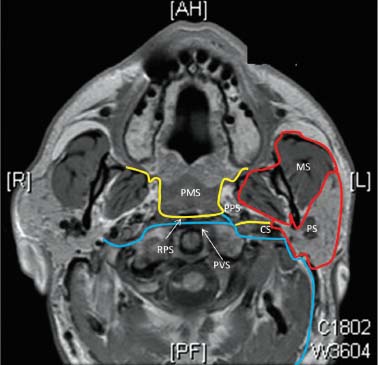
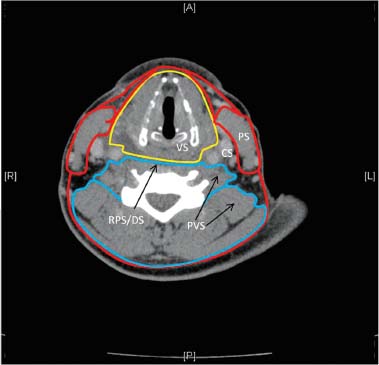
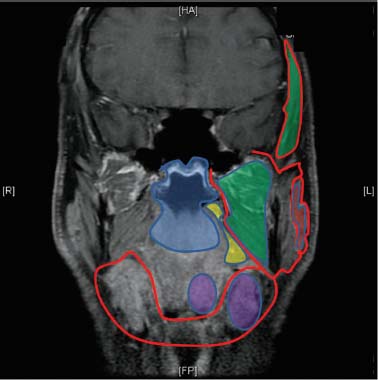
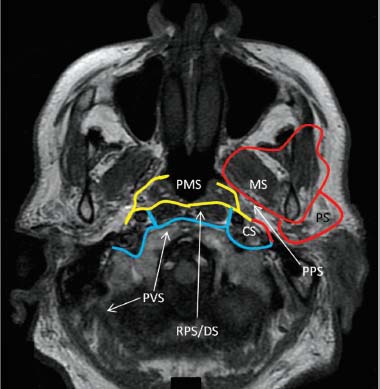
35 Core Messages • Understanding the anatomy and the relationships between the fasciae of the head and neck and their spaces is mandatory for comprehending the manner of spread of most infections and some tumors. • The cervical fascia is divided into superficial and deep layers, with the deep one further subdivided into superficial, middle, and deep layers. • The superficial fascia and the superficial layer of the deep fascia surround the entire neck. The middle layer of the deep cervical fascia encircles the center of the anterior neck to contain the viscera of the neck. The deep layer of the deep cervical fascia encircles the spine and the paraspinal muscles. • The cervical fascia divides the neck into several distinct spaces. The submandibular space corresponds to the submental and submandibular triangles. • There are four distinct spaces between the pharynx and the vertebral bodies. From anterior to posterior, they are (1) the visceral space, (2) the retropharyngeal space, (3) the danger space, and the (4) prevertebral space. Understanding the anatomy and the relationships between the fasciae of the head and neck and their spaces is mandatory for comprehending the manner of spread of most infections and some tumors. Proximity of the fascial spaces to various vital structures may cause devastating complications, such as airway obstruction, jugular septic thrombophlebitis, lung abscess, upper airway abscess rupture with asphyxiation, mediastinitis, pericarditis, and septic shock. As such, familiarity with the anatomy and interconnections of the fasciae and spaces of the head and neck is crucial for planning a surgical approach.1,2 Fascia does not have well-defined content and texture and varies in thickness and composition. Similarly, its origin and edges are arbitrary in most cases because fasciae may split to surround muscles, vessels, and nerves that have their own surrounding fascia and then merge with other fascial layers. As a result, the compartments they create (i.e., the fascial spaces) are mostly ill-defined areas of relatively loose connective tissues that vary in their content. Computed tomography (CT) and magnetic resonance imaging (MRI) revealed that certain fasciae restricted the growth of some tumors, whereupon knowledge of the anatomy of these fasciae opens the way to understand a disease process and predict its growth patterns. This chapter reviews the major anatomic descriptions of the fasciae and spaces of the head and neck.3 The fasciae of the head and neck are divided into superficial and deep layers (Figs. 35.1 to 35.3). The superficial cervical fascia (SCF) is a subcutaneous thick, well-defined layer of relatively loose connective tissue. SCF covers the head, face, and neck and contains the platysma, the muscles of facial expression, and portions of the anterior and external jugular veins. The deep cervical fascia (DCF) is thinner and contains denser, more discrete layers. The DCF travels along the neck below the skull base and encloses the muscles of the neck, as well as the mandible and the muscles of mastication and deglutition. The DCF is subdivided into three layers: (1.) the superficial layer of the deep cervical fascia (SLDCF), (2.) the middle layer of the deep cervical fascia (MLDCF), and (3.) the deep layer of the deep cervical fascia (DLDCF).4–6 The SCF consists of a loose connective tissue that underlies the skin of the head and neck. It contains sensory nerves, superficial vessels, and lymphatics. It extends from the superior aspect of the head down to the face where its fat content is dense, except around the eyelids. Between it and the periosteum of the calvarium, there is loose areolar tissue that permits motion of the muscles of facial expression and can hold large accumulations of fluid. Within the neck, it contains loose fatty tissue and the platysma muscle. The skin with SCF and the platysma muscle creates a unit that is interconnected by a system of fine connective tissue fibers and less well-defined muscular elements called the superficial musculoaponeurotic system (SMAS).7 The SMAS interlinks facial muscles with the dermis. It extends from the temporalis and frontalis muscles superiorly down to the platysma. Figure 35.1 Axial T1-magnetic resonance shows fascial spaces at the level of the nasopharynx. Three layers of the deep cervical fascia: superficial (red), middle (yellow), and deep (blue). Notice the relationship between spaces. From anterior to posterior: MS, masticatory space; PS, parotid space; PMS, pharyngeal mucosal space; CS, carotid space; PPS, parapharyngeal space; RPS, retropharyngeal space; DS, danger space; PVS, prevertebral space. The three layers of the DCF envelop the contents of the head and neck and form the deep neck spaces.8 The SLDCF is a well-defined sheet of fibrous tissue that completely envelops the neck. It arises from the ligamentum nuchae of the cervical vertebra and extends laterally and splits to enclose each trapezius muscle. It then crosses the posterior triangle of the neck and splits again to enclose each sternocleidomastoid (SCM) muscle. Anteriorly, it fuses and crosses the midline of the neck in front of the strap muscles as a single fascia. Just deep to the SCM, it contributes to the lateral aspect of the carotid sheath. Inferiorly in the midline, the SLDCF splits to attach the anterior and posterior aspects of the manubrium. Lateral to the sternum, the SLDCF attaches to the superior margin of the clavicle and extends to the spine of the scapula. The SLDCF contains most portions of the anterior and external jugular veins. Above the hyoid bone, the SLDCF extends superiorly to the lower border of the mandible. As it forms the floor of the submandibular space, it fuses and covers the anterior belly of the digastric and mylohyoid muscles. When the SLDCF reaches the mandible, the fascia divides into superficial and deep leaflets. These leaflets extend superiorly, enclosing the muscles of mastication and forming the masticator spaces. The superficial leaflet overlies the masseter muscle and attaches to the zygomatic arch. The fascia at this point splits once again to enclose the zygomatic arch, creating a small space over the superior surface of the arch that is filled with fat. The superficial leaflet then continues superiorly to overlie the temporalis muscle, attaching along the temporal ridge cranially and dorsally and along the lateral orbital margin ventrally. Anteriorly, the fascia covering the masseter muscle curves medially to attach to the mandible. The fascia covering the masseter muscle attaches to the buccinator fascia and to the maxilla, creating the masticator fat pad. This fat pad is intimately associated with the masticator space, and the fat has small projections into the pterygopalatine fossa along the lateral pterygoid muscle. The deep leaflet of the SLDCF extends cranially to form the medial or inner boundary of the masticator space. Figure 35.2 Axial T1-magnetic resonance shows fascial spaces at the level of the nasopharynx. Three layers of deep cervical fascia: superficial—red; middle—yellow; and deep—blue. Notice the relation between spaces. CS, carotid space; DS, danger space; MS, masticatory space; PMS, pharyngeal mucosal space; PPS, parapharyngeal space; PS, parotid space; PVS, prevertebral space; RPS, retropharyngeal space. Figure 35.3 Axial computed tomography shows infrahyoid fascial spaces. Three layers of the deep cervical fascia (DCF): superficial (red), middle (yellow), and deep (blue). Notice the relationship between spaces. Superficial and deep layers of the DCF merge at the ligamentum nuchae. CS, carotid space; DS, danger space; PS, parotid space; PVS, prevertebral space; RPS, retropharyngeal space; VS, visceral space. The MLDCF encloses the anterior neck. It has two parts, a muscular one, which encases the infrahyoid strap muscles (sternothyroid, sternohyoid, and thyrohyoid), and a visceral one, which envelops the trachea, larynx, pharynx, esophagus, and the thyroid gland. The muscular division extends inferiorly behind the sternum and then fuses with the pericardium and the great vessels in the superior mediastinum. Superiorly, it fuses with the thyroid cartilage and the hyoid bone. Laterally, the fascia extends to the sternum, clavicle, and scapulae. The visceral division lies posterior to the strap muscles and extends from the pharyngeal constrictor muscles and hyoid bone down into the anterior mediastinum to attach the fibrous pericardium and great vessels. The posterior-superior part of the MLDCF, also known as the buccopharyngeal fascia (BPF), extends from the skull base and follows the pharyngeal constrictors. This fascia is adherent to the muscular wall of the pharynx and the esophagus, and there is no real space between it and the viscera. The BPF encircles the posterior pharynx and forms the anterior wall of the retropharyngeal space. It splits to enclose the more cranial portion of the levator muscle, and a lateral leaflet of the BPF lies in close association with the lateral margin of the tensor veli palatini muscle. A thick fascial sheet extends inferiorly and posterolaterally to the styloid process from the posteroinferior edge of the tensor veli palatini muscle, fusing inferiorly with the fascia covering the styloglossus muscle. This fascial sheet thus closes the gap between the tensor veli palatini, the skull base, and the styloid process. Anteriorly, this fascia reaches the pterygomandibular raphe where it fuses with both the interpterygoid fascia and the BPF. This fascia contains the ascending palatine artery and vein. The DLDCF encloses the posterior contents of the neck. It originates posteriorly from the vertebral spinous processes and extends anterolaterally under the trapezius muscle enveloping the muscles of the posterior triangle of the neck floor. Laterally, the DLDCF extends between the middle and anterior scalene muscles after which it invaginates outward around the brachial plexus and subclavian artery. More laterally, it continues parallel to the axillary sheath. Medially, as the DLDCF reaches the anterior aspect of the vertebral bodies, it divides into the prevertebral fascia and the alar fascia. The alar fascia lies anteriorly to the prevertebral fascia and forms the posterior wall of the retropharyngeal space. It extends from the skull base down to the level of the C6-T4 vertebrae. The alar fascia is also the anterior wall of the danger space, which extends downward to the level of the diaphragm in the posterior mediastinum. The prevertebral fascia adheres directly to the vertebral bodies and cervical muscles and serves as the posterior wall of the danger space. The potential prevertebral space lies between the vertebral bodies and prevertebral fascia. It extends from the skull base down to the coccyx. Laterally, the DLDCF separates the lower neck and the thorax by extending from the transverse process of C7 to attach to the medial surface of the first rib, covering the dome of the pleura. The carotid sheath consists of contributions from all three layers of the DCF (Figs. 35.1 and 35.2). It contains the carotid artery, internal jugular vein, cervical sympathetic chain, and cranial nerves IX, X, XI, and XII. The inferior and middle portions of the carotid sheath originate from the SLDCF (from the fascia covering the SCM) and from the DLDCF. The upper portion is complex and formed by the SLDCF (from adjacent muscular fasciae), which forms the lateral wall; the DLDCF (alar and prevertebral fasciae), which forms the posterior wall; the cloison sagittale (either part of the DLDCF or the MLDCF), which forms the medial wall; and the stylopharyngeal aponeurosis (MLDCF), which forms the anterior wall. Some areas have overlapping that gives added strength, while there may be focal dehiscences, especially along the medial wall, in other areas. The fascial spaces are compartments between the fascial layers that are filled with loose connective tissue (Figs. 35.4 and 35.5). In some cases, these compartments represent potential spaces. Communication between spaces is variable and considered as normal anatomic variation.9,10 The suprasternal space is formed superior to the sternum when the enveloping fascia of the sternal heads of the SCM splits into two layers attached to the anterior and posterior surfaces of the manubrium. It extends from the sternum to halfway up the neck. The primary content of this space is fat and a communicating vein between the left and right anterior jugular veins. The visceral space contains the pharynx, cervical esophagus, trachea, thyroid gland, parathyroid glands, larynx, recurrent laryngeal nerves, and portions of the sympathetic trunk (Fig. 35.5). This region extends from the skull base down to the upper mediastinum. Its upper part is limited anteriorly by the BPF, posteriorly by the alar fascia, and laterally by the cloison sagittale fasciae. Its inferior portion is divided into two components. The anterior component is covered anteriorly by the strap muscles, laterally by the carotid sheaths, and posteriorly by the alar fascia. The posterior component is considered to have two subdivisions: an anterior pretracheal space and a more posterior retrovisceral space. These spaces communicate freely at the levels of the thyroid cartilage and the inferior thyroid artery. This connection explains why a retropharyngeal abscess can extend down into the pretracheal space and affect the thyroid gland and anterior mediastinum, and why a large thyroid goiter can extend behind the esophagus and grow either upward as a retropharyngeal mass or downward as a retroesophageal mass. Figure 35.4 Coronal T1-magnetic resonance image shows suprahyoid fascial spaces. MS (masticatory space) (green), has supra- and infrazygomatic compartments. The PPS parapharyngeal space (yellow) and the SLS sublingual space (medial purple) communicate at the posterior border of mylohyoid muscle. PS, parotid space (red); PMS, pharyngeal mucosal space (blue); SMS, submandibular space (lateral purple).
Head and Neck Fascial Spaces
Fasciae
Superficial Fascia
Deep Cervical Fascia
Superficial Layer of the Deep Cervical Fascia
Middle Layer of the Deep Cervical Fascia
Deep Layer of the Deep Cervical Fascia
Carotid Sheath
Fascial Spaces
Suprasternal Space
Visceral Space
Head and Neck Fascial Spaces
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


