Jugular Foramen Tumors
CHAPTER 82
The jugular foramen is the most complex foramen of the skull base. It both contains, and is surrounded by, important neurovascular structures. It is in a deep location, and surgical access poses difficulty for both otolaryngologists and neurosurgeons alike. Despite these anatomic challenges, impressive progress has been made in the surgical management of tumors of the jugular foramen. Advances in neuroradiology, the creation of formal skull base teams, and the utilization of microsurgical techniques have all contributed to a lowered surgical morbidity.
This chapter provides an overview of the relevant skull base anatomy needed to understand approaches to the jugular foramen. Because glomus jugulare tumors are, by far, the most common tumor of the jugular foramen, the bulk of the text is devoted to glomus tumors and their management. Although an overview of the surgical classification and treatment algorithm for jugular foramen tumors is provided, we have specifically described our surgical approach to these tumors.
Anatomy
The term jugular foramen is derived from the Latin terms for neck and aperture, respectively.1 Loosely speaking, this translates into “opening to the neck.” The jugular foramen truly is an opening to the neck, an avenue for passage of critical structures to and from the intracranial space of the posterior fossa to the neck.
OSSEOUS ANATOMY
The bony limits of this passageway are the petrous portion of the temporal bone and the condylar portion of the occipital bone.2 A fibrous bridge divides the jugular foramen in 75 to 92% of cadaveric specimens evaluated, and a bony septum in the remaining 8 to 25%.2 After the evaluation of human dry cadaveric skulls, it has been determined that the size of the jugular foramen is larger on the right than on the left in approximately 70% of specimens, larger on the left in 20%, and of the same size on both sides in 10%.2–5 The anterior margin of the jugular foramen is formed by the carotid ridge, which separates the jugular bulb from the C2 segment of the internal carotid artery (ICA)6 in the carotid canal.
CONTENTS OF JUGULAR FORAMEN
The critical structures traversing the jugular foramen are the sigmoid sinus and jugular bulb, the inferior petrosal sinus (IPS), meningeal branches of the ascending pharyngeal and occipital arteries, and cranial nerves (CN) IX, X, and XI (Fig. 82—001).
In addition, within the foramen are CN ganglia (superior and inferior ganglia of CN IX and X) and CN branches, including the tympanic branch of CN IX (Jacobson’s nerve) and the auricular branch of CN X (Arnold’s nerve). In close proximity to the jugular foramen are the ICA anteriorly and CN XII posteromedially.
COMPARTMENTS OF THE JUGULAR FORAMEN
Classically, the jugular foramen has been divided into two compartments, as described by Hovelacque in 1934.7 Later investigators called these two compartments the pars venosum (posterolaterally) and the pars nervosa (anteromedially).4, 8, 9 These names are misleading, as the pars venosum contains the jugular bulb, the posterior meningeal artery, as well as CN X and XI, and the pars nervosum contains CN IX and the inferior petrosal sinus. In 1997, Katsuta et al.2 divided the jugular foramen into three compartments: (1) the posterolateral sigmoid part (sigmoid sinus), (2) the interjugular or neural part (CN IX anteriorly, and CN X, XI posteriorly), and (3) the anteromedial petrosal part (inferior petrosal sinus). Their three-compartment (two venous and one neural or interjugular) classification system was based on observations made in 32 dry skulls and 33 cadaveric jugular foramina.2 The importance of compartmentalization of the jugular foramen is not to memorize a particular classification scheme, but rather to use these systems as a tool for understanding the anatomy of this region and how it affects the surgical approaches to pathological lesions.
VENOUS COMPONENT OF THE JUGULAR FORAMEN
The venous component of the jugular foramen consists of a large posterolateral venous channel (sigmoid part), which receives flow from the sigmoid sinus, and a smaller anterome-dial venous channel (petrosal part), which receives drainage from the IPS. The sigmoid sinus courses anteroinferiorly toward the jugular foramen, continuing as the jugular bulb, and then as the internal jugular vein. The dome of the jugular bulb is located approximately 2 mm inferior to the internal auditory canal. The dome of the jugular bulb may extend superiorly to the posterior wall of the internal auditory canal, in which case it is referred to as a “high jugular bulb”10, 11 (Fig. 82–2)).
The IPS courses on the intracranial surface of the petroclival fissure and enters the anteromedial (petrosal) part of the jugular foramen between CN IX and CN X. The IPS receives tributaries from the inferior petroclival vein (venous plexus in the carotid canal), venous plexus of the hypoglossal canal (anterior condylar vein), posterior condylar vein (emissary vein), and from the vertebral venous plexus. This confluence fills the anteromedial compartment of the jugular foramen, consisting of one or sometimes two main channels that receive drainage from smaller channels.
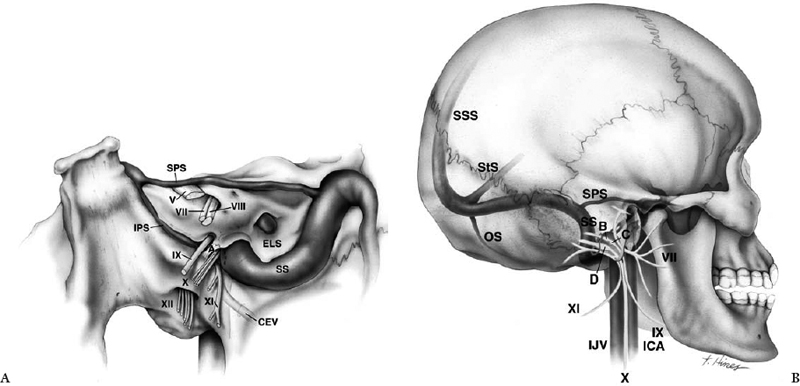
Figure 82-1 Endocranial and exocranial views of the jugular foramen. (A) Endocranial view shows cranial nerve (CN) IX is separated from CNs X and XI by a dural septum. The inferior petrosal sinus courses inferior to CN IX as the nerve enters the jugular foramen and courses between CN IX and X to drain into the anterior aspect of the jugular bulb. (B) Exocranial view of CNs and regional vascular relationships. CN XI courses posterolateral to the internal jugular vein. CN IX is lateral to CNs X and XI and is anchored to the internal carotid artery by a dense fibrous band. ICA, internal carotid artery; IPS, inferior petrosal sinus; SPS, superior petrosal sinus; SS, sigmoid sinus; StS, straight sinus; SSS, superior sagittal sinus; OS, occipital sinus; ELS, endolymphatic sac; CEV, condylar emissary vein; IJV, internal jugular vein; A, dural septum; B, superior ganglion of CN IX; C, inferior ganglion of CN IX; D, superior ganglion of CN X. (Reprinted with permission from the Mayfield Clinic.)
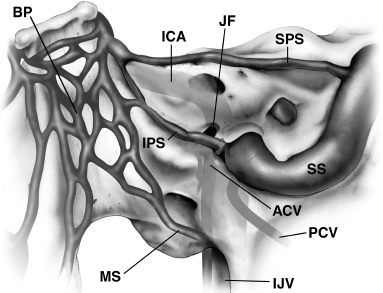
Figure 82-2Inferior petrosal sinus/anterior condylar vein complex. BP, basilar plexus; ICA, internal carotid artery; IPS, inferior petrosal sinus; JF, jugular foramen; SPS, superior petrosal sinus; SS, sigmoid sinus; ACV, anterior condylar vein; PCV, posterior condylar vein; MS, marginal sinus; IJV, internal jugular vein. (Reprinted with permission from the Mayfield Clinic.)
Shiu et al.12 described a classification system for the inferior petrosal sinus/anterior condylar vein complex that was further refined by Miller et al.13 In type I (45% of cases), the IPS drains directly into the jugular bulb and connects with the suboccipital and vertebral venous plexus via a small anterior condylar vein. In type II (24%), the IPS joins an anterior condylar vein of similar size before draining into the jugular bulb. Type III (24%) occurs when the IPS is formed of small venous channels connected to the jugular bulb. In type IV (7%), the IPS is not connected to the jugular bulb, but anastomoses directly with the vertebral and suboccipital venous plexi and may send a small tributary to the internal jugular vein. In summary, the IPS/anterior condylar vein complex forms an anastomosis with the jugular bulb in more than 90% of patients.
INTERJUGULAR COMPARTMENT AND CRANIAL NERVES
The junction of the anteromedial and posterolateral parts of the jugular foramen is a site of two bony prominences, the inter-jugular processes, on the opposing surfaces of the temporal and occipital bones. These processes are joined by a fibrous septum or, less commonly, an osseous bridge, which forms the inter-jugular septum between the anteromedial and posterolateral compartments. The dura over this septum has two characteristic perforations: the glossopharyngeal meatus (for CN IX) and the vagal meatus (for CN X and XI). The IPS empties into the jugular bulb between these two openings in approximately 65%, less commonly inferomedial to both openings, and rarely superolateral to them.13 The dura in the superolateral margins of the inter-jugular septum is characteristically thick, forming a lip, the plica occipitalis obliqua or jugular dural fold, which becomes less distinct inferomedially over the glossopharyngeal and vagal meatus.2
GLOSSOPHARYNGEAL NERVE
Cranial nerve IX arises from the medulla as three or four tiny filaments that quickly collect into one or, rarely, two rootlets passing forward and laterally, ventral to the choroid plexus, to penetrate the glossopharyngeal meatus.2, 14 Cranial nerve IX then turns abruptly anteroinferiorly and, as it traverses the jugular foramen, gives rise to the tympanic branch (Jacobson’s nerve) to the tympanic cavity. Along its course in the temporal bone, the tym-panic branch of CN IX has many swellings formed by ganglion cells, a potential site of origin for glomus tumors. Cranial nerve IX exits the jugular foramen between the ICA and internal jugular vein and descends lateral to CN X and XI. More distally, CN IX passes anteriorly to cross the lateral surface of ICA deep to the styloid process, where it divides into several branches.
VAGUS NERVE
Cranial nerve X is composed of multiple combinations of small and large rootlets, which are intimately associated with the rootlets of CN IX and XI. These rootlets enter the vagal meatus separated from the glossopharyngeal meatus by a dural septum. During its course in the jugular foramen, CN X gives the auricular branch (Arnold’s nerve), which ascends toward the mastoid segment of the facial nerve. Along its course, the auricular branch of CN X has many swellings formed by ganglion cells, which can give rise to glomus tumors. Cranial nerve X exits the jugular foramen vertically with intimate relation to CN XI. Cranial nerves X and XI exit the jugular foramen posterior to CN IX on the posteromedial wall of the internal jugular vein. The main trunk of CN X descends posterior to the ICA within the carotid sheath.2
SPINAL ACCESSORY NERVE
Cranial nerve XI has a cranial portion (4 to 16 rootlets) and a spinal portion (6 to 7 rootlets) from C1 to C6 dorsal to the dentate ligament. The cranial and spinal portions of CN XI enter the vagal meatus together; however, they may infrequently be separated by a dural septum. Cranial nerve XI may be indistinguishable from CN X in the jugular foramen. After exiting the foramen, CN XI descends obliquely and laterally between the ICA and internal jugular vein, and then posteri-orly across the lateral surface of the vein to reach the stern-ocleidomastoid and trapezius muscles. In 30% of specimens, CN XI descends alternatively on the medial surface of the internal jugular vein.2
HYPOGLOSSAL NERVE
Cranial nerve XII does not traverse the jugular foramen, but joins CN IX, X, and XI as they exit the foramen into the carotid sheath. After passing through the hypoglossal canal, CN XII courses adjacent to CN X and then separates from it and descends laterally in the interval between the ICA and internal jugular vein. At the level of the transverse process of the atlas, the main fibers of CN XII turn abruptly anteriorly along the lateral surface of the ICA en route to the tongue, whereas the remaining fibers, the ansa cervicalis, descend with the major vessels in the neck.
FACIAL NERVE
The vertical portion of the mastoid segment of the facial nerve in the fallopian canal, a critical structure in surgical approaches to the jugular bulb, is separated from the lateral wall of the jugular bulb by the retrofacial and infralabyrinthine air cells. The relationship between the mastoid segment of the facial nerve and the jugular bulb is variable.15 In approximately 60% of specimens at least one-half of the jugular bulb lies anterior to the facial nerve, and in the remaining 40% only one-third of the jugular bulb lies anterior to the facial nerve.15 The facial nerve exits the stylomastoid foramen about 5 mm lateral to the lateral margin of the jugular foramen or approximately midway between the styloid process and the anterior part of the digastric groove.
Tumor Classification
Glomus jugulare tumors are the most common tumors of the jugular foramen. Jugular schwannomas and meningiomas, although uncommon, are the other most common tumors affecting the jugular foramen, some series reporting the former and other series reporting the latter as the second most common.2, 14, 16 Chordoma,17, 18 chondrosarcoma,16, 19 chondroblastoma,16 cholesterol granuloma,20 epidermoid cyst,20 parotid neoplasm,16 adenocarcinoma,16 osteoblastoma,16 metastasis,21 plasmacytoma,22 sarcoidosis,23 fibrous dysplasia,24 chondromyxoid fibroma,25 non-Hodgkin’s lymphoma,26 and amyloidoma27 are among the other types of lesions reported in the jugular foramen.
Tumors of the jugular foramen may be either intrinsic, arising from within the foramen, or extrinsic, secondarily extending into the jugular foramen.14 Glomus jugulare is the classic intrinsic jugular foramen tumor, constituting 56 to 77% of jugular foramen tumors in reported series.14 Schwannomas and meningiomas rarely arise as primarily intrinsic jugular foramen tumors.14 Extrinsic tumors can penetrate the jugular foramen from four different directions: (1) superiorly, as a downward extension of intracranial schwannomas and meningiomas; (2) inferiorly, as an upward extension of cervical tumors such as glomus vagale tumors, adenocarcinomas, and schwannomas arising in the parapharyngeal space; (3) medi-ally, such as chordomas and chondrosarcomas of the petroclival region; and (4) laterally, from invasive temporal bone tumors such as squamous cell carcinoma and adenomatous tumors.14
Glomus Jugulare Tumors
HISTORY
In 1840 Valentin28 first described paraganglionic tissue near the origin of the tympanic nerve; this was followed in 1878 by Krause,29 who described the same tissue arising from the temporal bone. However, these early reports received little attention. Subsequently, in the Anatomic Records of 1941, Guild30, 31 was the first to use the term glomus body, but the significance of this tissue was unknown at that time. Shortly thereafter, in 1946, Rosenwasser32 described a “carotid body-like” tumor of the middle ear, followed 2 years later by Win-ship et al.33 coining the name glomus jugulare tumor. Through the 1940s and 1950s, several reports appeared in the literature, but the exact anatomic origin and behavior of this tissue was unknown.34 The terms chemodectoma and receptoma were used to refer to these glomus jugulare tumors because of their similarity to carotid body tumors, but unlike carotid body tumors, glomus jugulare tumors have no chemoreceptors.35 Paraganglionoma accurately reflects the origin of these tumors from the paraganglion cells. Nonchromaffin was added to the term paraganglionoma to convey the lack of positive silver staining by these tumors, but this was inaccurately interpreted to mean that these tumors were nonsecretory.36
In the history of the neurosurgical management of cranial neoplastic disease, glomus tumors of the jugular foramen and temporal bone are relatively new. In 1962, Alford and Gilford,36 in reviewing their own experience (11 cases) and the entirety of cases reported in the literature to date, found only 316 cases of glomus jugulare tumors. In this report, written in the era before modern imaging studies, they defined the natural history of this disease and described a detailed five-tiered classification system based on clinical signs and symptoms.
| Class | Description |
| A | Tympanic (4/23) |
| B | Tympanomastoid (7/23) |
| C | Infralabyrinthine (12/23) |
| D | Intracranial (1/12, recurrence of pt. with type C) |
| D1 | < 2 cm |
| D2 | > 2 cm |
*From Oldring and Fisch37 and Jenkins and Fisch.38
Series data: 23 patients, 5 M:18 F, mean age 48 years, range 20–69.
CLASSIFICATION SYSTEMS OF GLOMUS TUMORS
Two contemporary anatomically based classification systems of glomus tumors are commonly cited. The first is the four-tiered grouping of Oldring and colleagues37 of Zurich, first reported in 1979 and subsequently revised in later reports (Table 82-1). The second is the classification initially described in 1982 by Glasscock and Jackson39 of the Otology Group in Nashville. The latter classification divides glomus tumors into two main groups, glomus jugulare tumors and glomus tympanicum tumors. Each of these two main groups is further subdivided into four subgroups (Table 82-2). These classification systems serve as the standard language by which these lesions can be described. In addition, preoperative grading of glomus tumors that use these classification schemes and preoperative imaging studies has been shown to be a useful guide for choosing the appropriate surgical approach. Finally, the preoperative grade of the tumor according to these classification systems correlates with the likelihood of attaining a complete surgical resection and as a predictor of postoperative CN morbidity.14
| Type | Description |
| A. | Glomus tympanicum |
| I Small promontory mass | |
| II Fills middle ear | |
| III Extends into external auditory canal, with or without extension to ICA | |
| IV Glomus tympanicum | |
| B. | Glomus jugulare |
| I Small, jugular bulb, middle ear, mastoid | |
| II Extends under IAC, with or without intracranial extension | |
| III Extends to petrous apex, with or without intracranial extension | |
| IV Beyond petrous apex to clivus or infratemporal fossa, with or without intracranial extension |
*From Glasscock et al.39
BIOLOGY OF GLOMUS TUMORS
Pathology
Macroscopically, glomus jugular tumors are typically tan-gray to purple, encapsulated, vascular, and lobulated masses. Native glomus tissue and glomus tumors are derived from the embryological neural crest cells. Like the normal glomus tissue, glomus tumors are histologically indistinguishable from carotid body tumors and often display the histologic pattern referred to as Zellballen, with clusters of chief and sustentacular cells.5 Nuclear pleomorphism, hyperchromatism, and mitoses may not imply aggressive behavior. Rather, malignancy is defined as the presence of metastasis to an organ without paraganglia (versus multifocal) and occurs in fewer than 10% of cases.40 The distinction between multifocality and metastasis is illustrated by the example of a patient with a second glomus tumor in the lungs. The pulmonary lesion may not represent metastasis, as native glomus tissue is purported to occur in many locations, including the peribronchial tissue. Because of their slow growth, glomus tumors are somewhat insensitive to radiotherapy, but radiation does afford some degree of tumor control.
Anatomic Origin and Distribution of Glomus Tumors
Rockley and Hawke41 carefully studied the anatomic distribution of glomus bodies, and concluded that the division of glomus tumors into tympanicum or jugulare types is an arbitrary clinical classification, not reflecting the true anatomic distribution of glomus bodies. These workers proposed that “glomus bodies” are localized along the adventitia of the jugular dome, the tympanic branch of the glossopharyngeal nerve (Jacobson’s nerve), and the auricular branch of the vagus nerve (Arnold’s nerve).42 Tumors arising along Jacobson’s nerve or the promontory of the middle ear are of the glomus tympanicum type, whereas those arising proximal to Jacobson’s nerve in the inferior tympanic canaliculus (adjacent to the jugular bulb) are of the glomus jugulare variety. Glomus bodies located along the course of Arnold’s nerve adjacent to the facial nerve account for the occasional tumor in the descending facial canal.43 Rarely, tumor can arise from glomus tissue in the vagus nerve (i.e., glomus vagale).44
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


