Granular Myringitis and Tympanic Retraction Pockets
Richard M. Levinson
GRANULAR MYRINGITIS
Granular myringitis is a chronic vascular fibroproliferative and ulcerative dermatitis involving focal or diffuse areas of the tympanic membrane and adjacent canal wall (Fig. 15.1). Synonyms include chronic myringitis, polypoid myringitis, or myringitis granulosa.
Any condition resulting in desquamation and epithelial disruption of the squamous epithelium with exposure of the lamina propria can potentially incite this disorder. This includes local trauma from any source both direct and caustic, dermatologic conditions involving the external auditory canal, such as eczematoid or psoriatic-like skin disorders, or infectious agents. Numerous bacterial agents (Staphylococcus aureus, Staphylococcus epidermidis, Pseudomonas aeruginosa and Proteus mirabilis being the most common) and fungal agents (predominantly Candida) have been implicated. Suppression of reepithelialization with proliferation of inflammatory granulation from the lamina propria of the tympanic membrane ensues and the indolent course then follows (1, 2, 3).
Occult chronic suppurative otitis media may sometimes mimic granular myringitis. In this case a small perforation of the tympanic membrane may go unnoticed in the depths of the granulation tissue on the surface of the tympanic membrane only to be discovered after initiation of treatment or upon careful microscopic otoscopy with suction debridement.
The principal symptoms are mild otorrhea, muffled hearing, and occasional itching. The otologic examination typically reveals a cloudy mucoid discharge overlying an area of superficial granulation. There is no predilection for involvement of any particular location on the tympanic membrane. There is no evidence of perforation, and the drum moves well with pneumatic otoscopy.
If left untreated (or unsuccessfully treated), the clinical course may continue for months or years. Initial treatment should include debulking the granulations by either careful debridement with curettage, judicious chemical cautery (e.g., silver nitrate, trichloroacetic acid), or both. Prior to manipulation it may be necessary to locally anesthetize the area by injection technique (e.g., infiltrating the skin of the posterior canal wall with a xylocaine-epinephrine or marcaineepinephrine preparation utilizing a 30-gauge needle) or by applying topical anesthesia (e.g., iontophoresis technique, EMLA cream applied to the area). In many cases the area is strangely insensitive and no anesthetic is required. Water precautions should be instituted, and antibiotic-steroid eardrops should be used a minimum of twice daily. A culture of the area should be obtained to ensure that the chosen pharmacologic therapy is appropriately directed if one or two treatments are not successful in gaining control of the situation.
If three or four courses of therapy are unsuccessful, it is recommended that skin grafting be performed on an ambulatory basis. After anesthetizing the area, granulations are thoroughly removed. Removal of granulations extends down to the pars propria of the tympanic membrane and to the bone of the external canal. Thin skin grafts are harvested from the upper arm or medial surface of the auricle opposite the scapha with a razor blade, as described in Chapter 10, and are applied to the prepared recipient site. It is not necessary to trim the graft to exactly fit the recipient site, because overlapping areas will necrose. The ear canal is then packed firmly with the surgeon’s choice of packing (e.g., rosebud type, Merocel). The packing is gently removed in 2 weeks, and cleaning by aspiration is delayed another 2 weeks.
Granular myringitis that leads to stenosis will require more extensive surgery, including meatoplasty, canalplasty, and skin grafting, as described in Chapter 13.
RETRACTION POCKETS
A retraction pocket results from medial displacement of a portion (or all) of the tympanic membrane (Fig. 15.2). Synonyms include atelectatic retraction pocket, atelectatic otitis, adhesive otitis, myringomalacia, middle ear epidermatization, and marginal perforation pocket. If the pocket shows only mild medial displacement and is mobile on pneumatic otoscopy, it is deemed superficial and safe. A deep pocket implies significant extension into the mesotympanum or epitympanum. The epithelium of the retraction pocket may be fixed in position and immobile on pressure otoscopy. Unsafe pockets prone to complications fall into this category. Various grading systems have been proposed for classifying the severity of retraction (4,5). The formation and medial migration of a retraction pocket is a dynamic process and may arrest at any stage (6,7). A seemingly safe and stable retraction pocket, however, may progress and develop complications after years of quiescence.
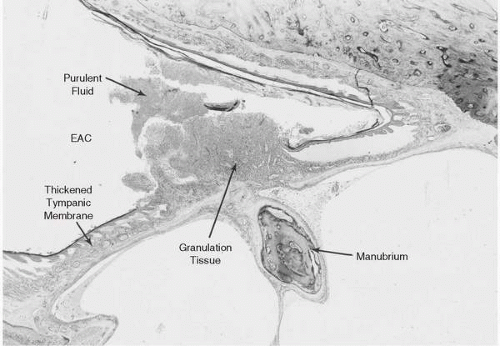 FIG. 15.1 Granular myringitis. A horizontal section through the tympanic membrane of the right ear of a 32-year-old man shows focal granular myringitis. There is a proliferation of highly vascular granulation tissue with ulceration of the skin and seropurulent discharge. The pars propria of the tympanic membrane is intact. There is inflammatory thickening of the subcutaneous layer of the tympanic membrane. EAC, external auditory canal. 19.2X. |
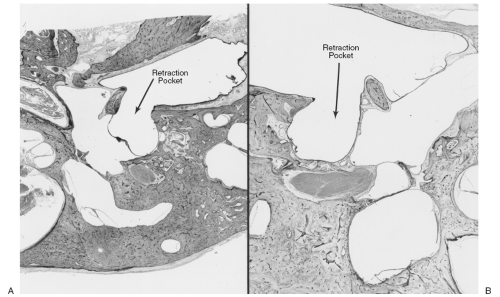 FIG. 15.2 Retraction pockets. A: A clean, dry posterior retraction pocket in the right ear of a 67-year-old man. The lining membrane is adherent to the posterior wall of the mesotympanum. 3.4X. B: A clean, dry posterior retraction pocket is seen in the left ear of a 47-year-old woman. The lining membrane is adherent to the posterior wall of the mesotympanum and the fallopian canal. 5.5X. |
The pathogenesis of an atelectatic retraction pocket is related to weakening of the structural integrity of the drum from deterioration of the lamina propria associated with negative middle ear pressure from either eustachian tube dysfunction or sniff-induced negative pressure. Middle ear or epitympanic adhesions may also play a role.
Symptomatic retraction pockets include those that are infected and producing otorrhea and granulation tissue and those that retain keratin debris with or without infection (Fig. 15.3). Deep retraction pockets harboring squamous debris and infection often cause osteitis of the ossicles, particularly the long process of the incus. Occasionally a dry, clean pocket will result in ossicular destruction over time.
Conservative management is reserved for those retraction pockets whose limits can be completely visualized, are not fixed to underlying structures, and are causing no complications. Autoinflation techniques for eustachian tube promotion, home politzerization, nasal balloon inflation with an olive-tip adapter, and encouragement for blowing rather than sniffing should be considered. Polyethylene (PE) tube placement can be helpful; however, it is common for the retraction pocket to recur after tube extrusion.
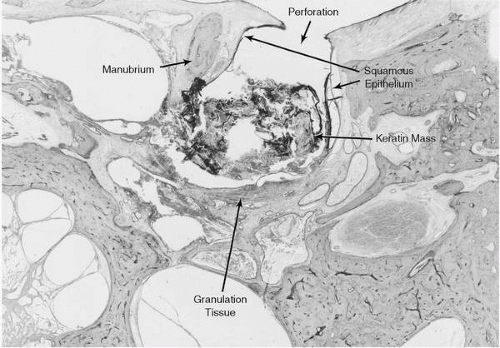 FIG. 15.3 Retraction pocket and cholesteatoma. The right ear of this 67-year-old man shows a deep posterior retraction pocket that is lined partly by squamous epithelium and partly by granulation tissue. A keratin mass (cholesteatoma) occupies the posterior mesotympanum. 10.5X. |
Surgical intervention for a retraction pocket is indicated for one or more of the following reasons: (i) persistent or recurrent otorrhea, (ii) persistent granulation tissue (often associated with otorrhea or bone destruction), (iii) ossicular destruction with significant conductive hearing loss, (iv) non-cleansing pocket whose limits cannot be adequately assessed on microscopic otoscopy, and (v) overt cholesteatoma.
Numerous surgical remedies have been proposed for retraction pockets, including simple excision of the retraction pocket with no reconstruction and concurrent PE tube placement in an unaffected part of the drum (8,9), myringoplasty/tympanoplasty with fascia (with and without a PE tube), and canalplasty to prevent accumulation of squamous debris (10). Recurrence, however, is not uncommon, and ongoing treatment is often necessary.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


