Purpose
To determine whole-eye high-order aberrations (HOAs) in pseudophakic eyes after Descemet stripping endothelial keratoplasty (DSEK) for Fuchs dystrophy, and to establish relationships between graft thickness, HOAs, and visual acuity.
Design
Cross-sectional study.
Methods
Whole-eye HOAs were measured in pseudophakic eyes at intervals through 24 months after DSEK, and in otherwise healthy pseudophakic control eyes implanted with the same type of spherical intraocular lens. Wavefront errors were assessed by a Hartmann-Shack aberrometer over a 4-mm-diameter optical zone. In DSEK eyes, central graft thickness and stromal graft folds were measured using confocal microscopy in vivo, and best-corrected visual acuity (BCVA) was determined by the electronic Early Treatment of Diabetic Retinopathy Study method.
Results
Total HOAs at 24 months after DSEK (0.28 ± 0.11 μm, mean ± SD, n = 17) were higher than those in pseudophakic controls (0.16 ± 0.07 μm, n = 25, P < .001); specifically, trefoil and quadrafoil were higher after DSEK. At 24 months, total HOAs (r = 0.69, P < .001) and graft folds (r = 0.41, P = .02) were correlated with central graft thickness, and BCVA was correlated with total HOAs (r = 0.39, P = .01) but not with graft thickness (r = −0.24, P = .20, n = 27).
Conclusions
Whole-eye HOAs are higher after DSEK compared to untreated corneas. Thicker grafts are associated with increased HOAs and more graft folds, suggesting that the donor lenticule contributes, in part, to the wavefront errors. Although BCVA is weakly related to total HOAs after DSEK, it is not related to graft thickness.
Descemet stripping endothelial keratoplasty (DSEK) is currently the preferred technique of corneal transplantation for endothelial disease. The success and rapid adoption of this technique can be attributed to distinct advantages over penetrating keratoplasty (PK), including better uncorrected visual acuity, more predictable postoperative refractive errors, and improved globe integrity. In addition, graft survival, which is the standard measure of success for corneal transplantation, at 5 years is similar to that after PK, and endothelial cell loss appears to be lower. Despite these advantages, quality of vision often remains degraded compared to normal, with best-corrected visual acuity (BCVA) often being less than 20/20 and disability glare being higher than normal. In fact, poor vision after DSEK has been suggested to be a leading cause of graft replacement during the first 5 postoperative years.
After DSEK for Fuchs dystrophy, we found that the large and small angle domains of the point-spread function were degraded compared to otherwise normal pseudophakic eyes. Degradation of the large angle domain was expected because of increased forward scatter that causes disability glare, whereas degradation of the small angle domain suggested that increased high-order aberrations (HOAs) might also degrade visual function after DSEK. In this study, we examined HOAs directly in DSEK patients; the goal of this study was to compare whole-eye HOAs in pseudophakic eyes after DSEK to those of age-matched, otherwise normal pseudophakic eyes implanted with the same type of spherical intraocular lens. We also assessed the relationships between HOAs, visual acuity, graft thickness, and stromal graft folds detected by confocal microscopy in vivo. Graft folds appear as dark striae in confocal images of the deep stroma, and may indicate a mechanical irregularity in the stroma that affects the curvature of the posterior corneal surface. Thus, in this study, we tested the hypothesis that thicker grafts were associated with more graft folds and increased HOAs.
Methods
Subjects
Subjects in the DSEK group were part of a prospective, observational study of DSEK for Fuchs dystrophy and were recruited from patients attending the Department of Ophthalmology at Mayo Clinic, Rochester, Minnesota. Subject age was 67 ± 10 years (mean ± standard deviation; range: 41–87 years), and all eyes were pseudophakic after DSEK with the graft prepared by a mechanical microkeratome. Forty-six eyes (40 subjects) were examined at 6 months, 36 eyes (29 subjects) were examined at 12 months, and 27 eyes (24 subjects) were examined at 24 months after DSEK.
Data from eyes in the DSEK group were compared to data from eyes of subjects in 2 control groups. The first control group included 25 pseudophakic but otherwise normal eyes of 17 subjects at 5 ±11 months (range: 1–60 months) after cataract surgery, and was age-matched to the DSEK group (70 ± 7 years; range: 55–83 years). The pseudophakic eyes were implanted with the same type of spherical intraocular lens (Acrysof SA60AT; Alcon Laboratories Inc, Fort Worth, Texas, USA) as in the DSEK group, and were controls for whole-eye HOAs. The second control group included 36 young normal, untreated eyes of 18 subjects who had undergone confocal microscopy as part of another study and served as controls for graft folds; age was 43 ± 7 years (range: 29–55 years).
Subjects were excluded if they had corneal scarring or disease (except for haze related to Fuchs dystrophy in the DSEK group), diabetes, glaucoma, or significant vitreous floaters, or if their vision was impaired because of maculopathy, optic neuropathy, or amblyopia. Pseudophakic eyes were excluded if they had posterior capsular haze.
Surgical Procedures
The technique for DSEK has been described previously and involved a 5- to 6-mm sutured scleral tunnel incision and 3 to 4 full-thickness host paracentral corneal venting incisions. All grafts were prepared using a mechanical microkeratome; grafts were inserted into the anterior chamber using a folding technique. When cataract surgery was performed in combination with DSEK, the same scleral incision was used for cataract removal by phacoemulsification and for intraocular lens insertion. Of the 46 eyes examined at 6 months, 38 eyes had undergone simultaneous DSEK and phacoemulsification, whereas 8 eyes had undergone DSEK alone after previous phacoemulsification.
Pseudophakic eyes in the control group received cataract extraction by phacoemulsification and intraocular lens insertion through a 2.75- to 3-mm clear corneal sutureless incision. All surgeries were uncomplicated and were without significant postoperative corneal edema.
Ocular Aberrations
Whole-eye HOAs were measured using a Hartmann-Shack aberrometer (VISX Wavescan, Santa Ana, California, USA). Subjects self-fixated on a target within the aberrometer during wavefront acquisition. The highest-quality examination with the largest wavefront (pupil) diameter, as determined by the software, was selected by 1 masked observer (L.S.S.). Wavefront errors were calculated using VOLCT (Sarver and Associates Inc, Carbondale, Illinois, USA) over a 4-mm-diameter optical zone, and were decomposed into Zernike polynomials to the sixth order. The root mean square (RMS) of all aberrations in orders 3 through 6 were calculated from the Zernike coefficients, as were the RMS of spherical aberration (Z04)(Z04)
( Z 4 0 )
, coma (Z−13,Z13)(Z−13,Z13)
( Z 3 − 1 , Z 3 1 )
, trefoil (Z−33,Z33)
( Z 3 − 3 , Z 3 3 )
, and quadrafoil (Z−44,Z44)
( Z 4 − 4 , Z 4 4 )
. Aberrometry was attempted in only 23 eyes at 6 months, 31 eyes at 12 months, and 24 eyes at 24 months after DSEK, and in all pseudophakic control eyes.
Confocal Microscopy and Graft Folds
Central corneas were examined using a confocal microscope (ConfoScan 4 with z-ring adapter; Nidek Technologies, Fremont, California, USA) to measure graft thickness and folds in eyes after DSEK, and to measure deep stromal folds in the young, normal corneas. The microscopy technique has been described in detail previously. The best full-thickness scan through the cornea was selected for analysis, and graft thickness was calculated using the graph of intensity of the confocal images through the cornea.
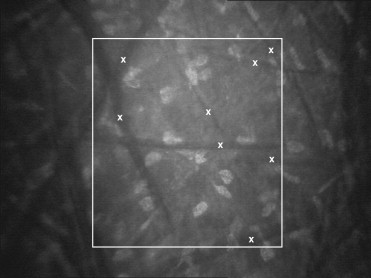
Graft folds were assessed from confocal images by 1 masked observer (C.B.N.). In each image, all folds that were visible within a central rectangle (215 μm × 242 μm; area, 0.052 mm 2 ) were identified and marked using a point-and-click method ( Figure 1 ). This region of the confocal image had the most consistent brightness, and visibility of folds decreased outside of this area. Folds were marked only once in any frame but were marked again if they appeared in consecutive frames. The folds index was the sum of the number of folds per frame (weighted for the distance, registered by the z-ring adapter, between consecutive frames) between the interface and the endothelium after DSEK, or between the endothelium and 160 μm (the mean central graft thickness after DSEK) anterior to the endothelium in untreated corneas.