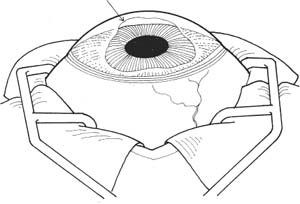
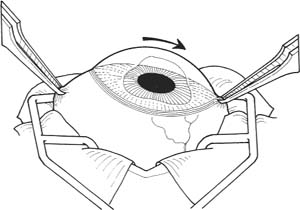
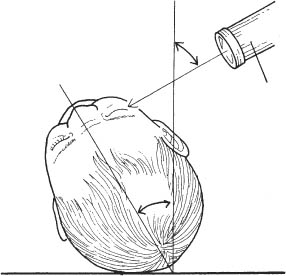
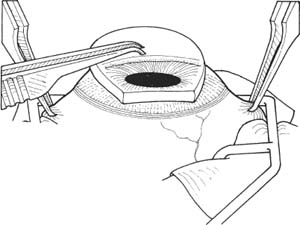
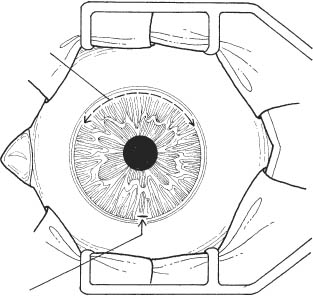
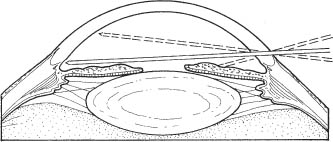
44 See Chapter 3. 1. Treatment of primary congenital glaucoma is usually surgical. Medical therapy is usually a temporizing measure before surgery. 2. Educate the parents about the possibility of multiple operations and frequent follow-up visits. 3. Perform a thorough preoperative examination of the patient in the office. Intraocular pressure (IOP) should be accurately determined in the office, as many drugs used during an examination under anesthesia alter the IOP. 4. Rule out nasolacrimal duct obstruction as a cause of epiphora. 5. Clear as much corneal edema as possible with medical treatment to lower the eye pressure. Use oral acetazolamide if needed. Goniotomy can be done with greater accuracy through a clearer cornea. 6. Apply a topical antibiotic ointment to both eyes the evening before surgery. 7. As long as an accurate eye pressure has already been obtained, a drop of 1% pilocarpine 30 minutes prior to surgery will protect the lens from the goniotomy knife. Figure 44.1 1. Anesthesia: General anesthesia. If an accurate IOP was not obtained in the office, it is imperative to obtain a pressure as soon as possible after induction of anesthesia. Many barbiturates and inhalational anesthetics decrease the eye pressure, and ketamine can increase the pressure. 2. Once pressure is obtained, the patient is intubated. 3. Perform an examination under anesthesia. Measure the corneal diameters and perform gonioscopy. Examination of the optic nerve can be done through an undilated pupil with a direct ophthalmoscope through the Koeppe lens. 4. Select the area where the goniotomy will be performed. Figure 44.2 5. If the cornea is cloudy, a drop of proparacaine is place on the eye. A small amount of alcohol is painted over approximately one fourth of the cornea, 180 degrees away from the side of the angle to undergo goniotomy. After 10 seconds, the alcohol is irrigated away, and the epithelium is scraped away with a #15 Bard-Parker blade (Fig. 44.2). Care should be taken to preserve the limbal epithelial cells. 6. Prep and drape. 7. The surgeon is positioned to face the angle where the surgery will be performed. 8. The assistant will be opposite the surgeon. 9. Place the lid speculum. 10. Fixation of the eye: Figure 44.3 a. Castroviejo forceps are used to grab the conjunctiva near the limbus at 6 o’clock, and the eye is infra-ducted (Fig. 44.3). A muscle hook can alternatively be used to infraduct the eye. b. Elschnig-O’Connor locking fixation forceps are used to lock the superior rectus. c. The eye is then supraducted. d. The other Elschnig-O’Connor locking fixation forceps are used to lock the inferior rectus. e. The lid speculum is removed. f. The two locking fixation forceps are handed to the assistant to position the globe. 11. Positioning of the head: Figure 44.4 a. The patient’s head is tilted 30 degrees away from the surgeon (Fig. 44.4). This facilitates the surgery and more easily allows removal of any air bubbles under the lens. Figure 44.5 Figure 44.6 b. Barkan gonioscopy lens is placed on the cornea (Figs. 44.5 and 44.6). BSS is placed under the lens. Optional: Use Goniosol with lens. 12. Entry of the goniotomy knife into the anterior chamber. a. The assistant may need to provide a slow and almost imperceptible movement of the eye toward the knife as it enters the eye to provide some counterresistance as the entered knife may push the eye away from the surgeon. b. The knife starts to enter the anterior chamber through the cornea ~1 mm from the limbus. The entry site is 180 degrees away from the center of the area of angle to have surgery (Fig. 44.7). c. As the knife passes through the cornea, the surgeon should shift his or her view through the Barkan operating lens. The knife should be seen entering the anterior chamber. Figure 44.7 Figure 44.8
Goniotomy and Trabeculotomy
 Goniotomy
Goniotomy
Indications
 Primary congenital glaucoma
Primary congenital glaucoma
 Other primary developmental glaucomas
Other primary developmental glaucomas
 Pediatric secondary glaucomas
Pediatric secondary glaucomas
 Prevention of glaucoma secondary to aniridia
Prevention of glaucoma secondary to aniridia
Preoperative Procedure
Instrumentation
 Pilocarpine 1% (optional)
Pilocarpine 1% (optional)
 Antibiotic ointment
Antibiotic ointment
 Proparacaine hydrochloride
Proparacaine hydrochloride
 Alcohol containing red dye
Alcohol containing red dye
 Handheld tonometer (e.g., Perkins)
Handheld tonometer (e.g., Perkins)
 Calipers
Calipers
 Koeppe gonioscopy lens
Koeppe gonioscopy lens
 Handheld microscope
Handheld microscope
 Barkan handheld light
Barkan handheld light
 Direct ophthalmoscope
Direct ophthalmoscope
 No. 15 Bard-Parker blade
No. 15 Bard-Parker blade
 Binocular loupes
Binocular loupes
 Headlight or operating microscope
Headlight or operating microscope
 Lid speculum
Lid speculum
 Elschnig-O’Connor locking fixation forceps
Elschnig-O’Connor locking fixation forceps
 Castroviejo 0.3 mm forceps
Castroviejo 0.3 mm forceps
 Muscle hook
Muscle hook
 Barkan operating gonioscopy lens, small and large
Barkan operating gonioscopy lens, small and large
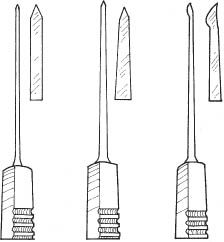
 Goniotomy knife (nontapered Swan, tapered Swan, or Barkan) (Fig. 44.1). (Note that the figure shows these knives in this order, from left to right.)
Goniotomy knife (nontapered Swan, tapered Swan, or Barkan) (Fig. 44.1). (Note that the figure shows these knives in this order, from left to right.)
 10–0 Vicryl
10–0 Vicryl
 Needle holder
Needle holder
 Tying forceps
Tying forceps
 Vannas scissors or fine suture scissors
Vannas scissors or fine suture scissors
 Weck-Cel sponges
Weck-Cel sponges
 Pediatric eye shield
Pediatric eye shield
Operative Procedure
 Balanced salt solution (BSS)
Balanced salt solution (BSS)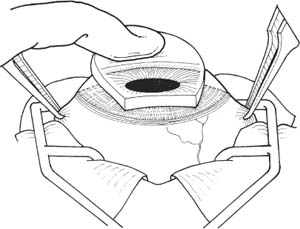
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


