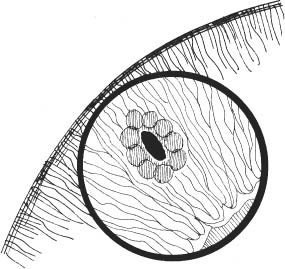
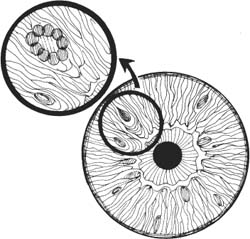
33 1. Examine anterior chamber angle with gonioscopy lens to assess degree of angle closure and anterior chamber depth. 2. Constrict pupil with pilocarpine 1% 30 minutes before procedure. 3. Place one drop of α-adrenergic agonist (e.g., brimonidine tartrate 0.10%, [Alphagan P, Allergan, Inc., Irvine, CA, US]). 1. Apply topical anesthetic (e.g., proparacaine). 2. Place Abraham lens with methylcellulose solution. 3. Select iridotomy site: a. Superonasal or superotemporal peripheral iris, approximately two thirds of distance from pupillary margin to limbus. b. Select iris crypt for easier penetration. c. In shallow anterior chamber, choose site where iris is most distant from cornea (to prevent endothelial trauma). d. Choose site as peripheral as possible but central to arcus senilus to facilitate visualization. 4. Focus at base of iris crypt, ensuring that laser is not aimed at macula or optic nerve. Figure 33.1 5. Apply stretch burns (Fig. 33.1). a. Approximately four to eight overlapping burns centered around planned penetration site. b. Laser parameters: i. Spot size: 200 μm. ii. Duration: 0.2 seconds. iii. Power: 100–200 mW. Figure 33.2 6. Apply penetrating burns (Fig. 33.2): Note: there are variations in parameters, depending on iris color. a. Aim at center of stretch burns. b. Laser parameters: i. Spot size: 50 μm. ii. Duration: 0.1 sec. iii. Power: 500–1500 mW (adjust as iris reaction indicates). c. Apply burns directly over each other until penetration is achieved. d. Number of applications required averages ~25 but may be more than 100. 7. Verify patency by visualizing anterior lens capsule or vitreous (in aphakes) directly through iridotomy with slit beam. (A red reflex by retroillumination does not confirm patency.) 8. When iris is penetrated, enlarge iridotomy by chipping away at its edges. a. Laser parameters: i. Spot size: 50 μm. ii. Duration: 0.05–0.1 sec. iii. Power: 500 mW. b. Do not aim laser directly through iridotomy to avoid damaging lens. 1. Prepare eye and select iridectomy site as described for drumhead method. 2. Focus laser at base of selected iris crypt. 3. Perform iridotomy using the following parameters: a. Spot size: 50 μm. b. Duration: 0.1 sec. c. Power: 500–1500 mW. (Adjust as iris reaction indicates.) 4. Apply burns directly over each other until penetration is achieved. 5. Verify patency of iridotomy with slit beam. 6. Upon achieving patency, enlarge iridotomy and remove residual pigment by chipping away at edge of opening using the following parameters. a. Spot size: 50 μm. b. Duration: 0.05–0.1 sec. c. Power: 500 mW. 1. Apply topical anesthetic (e.g., proparacaine). 2. Place Abraham lens with methylcellulose solution. 3. Select iridotomy site as described in argon laser drumhead method (see step 3, above) 4. Focus Helium-Neon laser aiming beam at desired site. 5. Optional: Apply stretch/cautery burns with argon laser. (May decrease bleeding caused by subsequent YAG applications.) a. Appl ~4–8 overlapping burns. b. Laser parameters. i. Spot size: 200 μm. ii. Duration: 0.2 sec. iii. Power: 100–200 mW. 6. Perform YAG laser treatment. a. Power: ~4–8 mJoules (start at 4 mJoules). b. May need to wait a few minutes between applications while debris disperses away from site. c. Apply 1–10 applications until patency is achieved. Note: YAG laser iridotomies have less propensity for late closure than do argon laser iridotomies. 7. If bleeding occurs at laser site, apply brief pressure to the eye with contact lens. 1. Reexamine angle with gonioscopy lens to assess effect of laser treatment on depth of anterior chamber. 2. Apply steroid drops (e.g., prednisolone acetate 1%) 4 times per day for 1 week, then taper to treat inflammation. 3. Place 1 drop of α-adrenergic agonist (e.g., brimonidine tartrate 0.10% [Alphagan P, Allergan, Inc.]) after laser treatment for prophylaxis against intraocular pressure spikes. 4. Continue pilocarpine 1% every 6 hours if unsure of iridotomy patency and if angle closure remains a possibility. 5. If iridotomy is patent and inflammation is severe, dilate pupil (e.g., cyclopentolate 1%) to avoid posterior synechiae. 1. Measure IOP 1 hour postlaser to check for pressure elevation. 2. Follow-up in 1 week to measure intraocular pressure (IOP) and examine iridotomy site. 3. Routine follow-up every 3 to 6 months thereafter. 1. Iritis 2. Hyphema (more common with YAG laser) 3. Transient elevation of intraocular pressure. 4. Closure of iridotomy (more common with argon laser) 5. Lens damage (localized) 6. Localized corneal endothelial damage: shattered glass appearance. 7. Retinal damage 1. Identify landmarks. 2. If angle is narrow, a laser iridotomy or gonioplasty may be performed initially to facilitate laser trabeculoplasty. 3. Apply one drop of 1% pilocarpine to stretch iris. 1. Apply topical anesthetic (e.g., proparacaine).
Glaucoma Laser Procedures
 Laser Iridotomy
Laser Iridotomy
Indications
 Relief of pupillary block in eyes with primary angle closure glaucoma
Relief of pupillary block in eyes with primary angle closure glaucoma
 Prophylaxis in eyes with anatomy predisposing toward angle closure
Prophylaxis in eyes with anatomy predisposing toward angle closure
 Aphakic or pseudophakic pupillary block
Aphakic or pseudophakic pupillary block
 Pupillary seclusion with iris bombe
Pupillary seclusion with iris bombe
 Selected cases of chronic or secondary angle closure glaucoma
Selected cases of chronic or secondary angle closure glaucoma
 Specific indications for use of laser rather than surgical iridectomy:
Specific indications for use of laser rather than surgical iridectomy:
 Treatment of imperforate surgical iridectomy
Treatment of imperforate surgical iridectomy
 Treatment of nanophthalmic eyes that frequently develop severe choroidal effusions with invasive procedures
Treatment of nanophthalmic eyes that frequently develop severe choroidal effusions with invasive procedures
 Prophylactic treatment of the fellow eye in ciliary block glaucoma
Prophylactic treatment of the fellow eye in ciliary block glaucoma
Preoperative Procedure
Instrumentation
 Argon, Nd:YAG, or Diode laser
Argon, Nd:YAG, or Diode laser
 Abraham iridotomy lens with peripheral 66 diopter button
Abraham iridotomy lens with peripheral 66 diopter button
Operative Procedure
Argon or Diode Laser
Technique 1: Drumhead method
Technique 2: Chipping away method
Nd:YAG Laser
Postoperative Procedure
Follow-up Schedule
Complications
 Laser Trabeculoplasty
Laser Trabeculoplasty
Indications
 Chronic open angle glaucoma uncontrolled by maximally tolerated medical therapy.
Chronic open angle glaucoma uncontrolled by maximally tolerated medical therapy.
 Glaucoma patients who are noncompliant with medications.
Glaucoma patients who are noncompliant with medications.
 Selected secondary open angle glaucomas uncontrolled by medical therapy, for example:
Selected secondary open angle glaucomas uncontrolled by medical therapy, for example:
 Pseudoexfoliative glaucoma.
Pseudoexfoliative glaucoma.
 Pigmentary glaucoma.
Pigmentary glaucoma.
 Laser trabeculoplasty is not useful for the angle closure or inflammatory glaucomas.
Laser trabeculoplasty is not useful for the angle closure or inflammatory glaucomas.
Preoperative Procedure
Examine Anterior Chamber Angle with Gonioscopy Lens
Instrumentation
 Argon green or blue-green or diode laser
Argon green or blue-green or diode laser
 Goldmann 3-mirror contact lens or similar gonioscopy lens.
Goldmann 3-mirror contact lens or similar gonioscopy lens.
Operative Procedure
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


