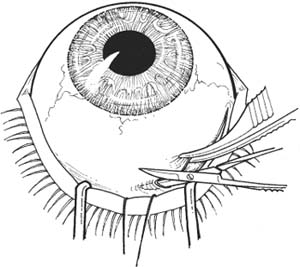
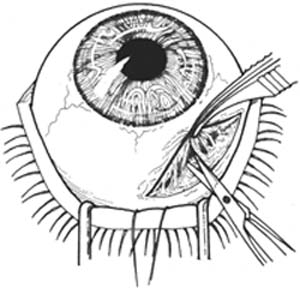
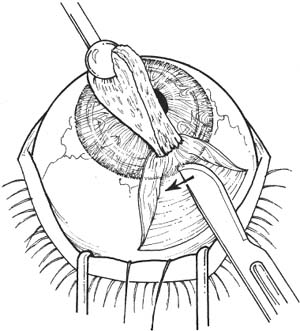
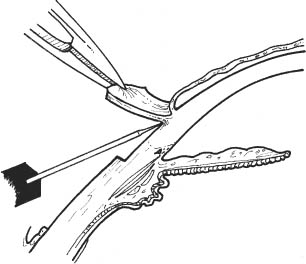
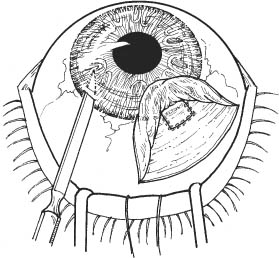
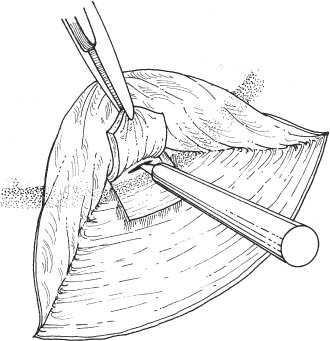
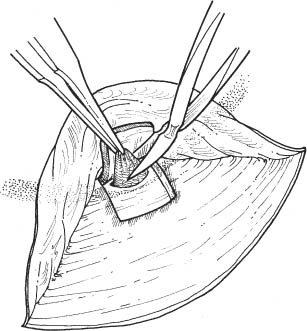
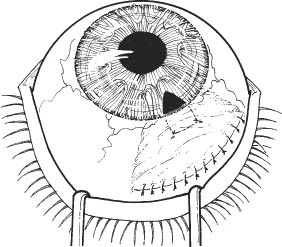
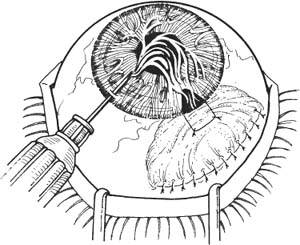
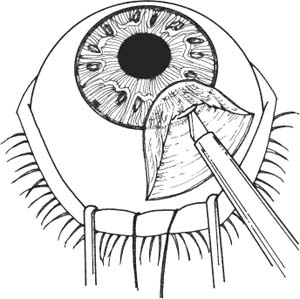
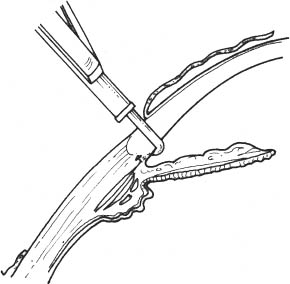
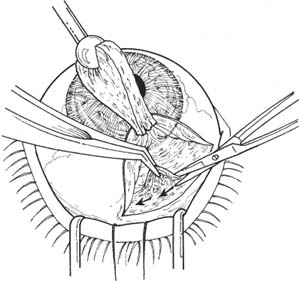
30 Glaucoma uncontrolled by maximally tolerated medical therapy and by laser trabeculoplasty. See Chapter 3. 1. Preoperative intraocular pressure (IOP) should be < 30 mm Hg. If the IOP is too high, intravenous or oral osmotics may be used. 2. Some medications used to treat glaucoma can, theoretically, compromise the prognosis of the filtration bleb. Therefore, they may be discontinued preoperatively. This should only be done, however, if adequate IOP control can be maintained without these medications or with substitute medications. The following agents are listed in the order of priority in which they should be stopped. a. Discontinue cholinesterase inhibitors (e.g., phospho-line iodide) 2 weeks preoperatively to decrease bleeding and postoperative inflammation. b. Discontinue carbonic anhydrase inhibitors 1–2 days preoperatively to increase aqueous flow through bleb. c. If IOP allows, discontinue β-blockers 1–2 weeks preoperatively, because decreased aqueous flow may compromise the bleb. d. Discontinue epinephrine, dipivefrin, apraclonidine, brimonidine, and latanoprost or other prostaglandin analogues 1 week preoperatively to decrease pre- and postoperative conjunctival injection and intraocular inflammation in the case of the prostaglandin analogues. 3. The eye should be as quiet as possible preoperatively to enhance the prognosis for successful filtration. a. Optional: Steroid drop 4 times per day to every hour preoperatively to decrease postoperative inflammation. b. Optional: Oral steroids (e.g., prednisone 80 mg) starting 1 day preoperatively. 1. Anesthesia: Retrobulbar or peribulbar injection plus lid block. May use general anesthesia if preferred, and for younger or uncooperative patients, hearing or mentally impaired patients, or those with language obstacles 2. Prep and drape. a. Use povidone-iodide 5% on a cotton-tipped applicator to gently clean eyelashes and lid margins. b. Place 1 or 2 drops of povidone-iodide in the conjunctival fornix. 3. Place lid speculum. 4. Place a 4–0 silk bridle suture under superior rectus tendon. Be careful not to injure conjunctiva (Kalt needle holder, Elschnig forceps). Alternatively place a 7–0 Vicryl braided suture through the peripheral cornea for traction. 5. Select position for filter placement, usually in supero-temporal or superonasal quadrant in area of least inflamed or scarred conjunctiva. Superonasal placement leaves room for subsequent cataract surgery if necessary. 6. Prepare limbus-based conjunctival flap. Note: Always handle conjunctiva gently and at the edges. Use nontoothed forceps. Figure 30.1 a. Incise superior bulbar conjunctiva for ~90 degrees, 10 mm posterior to the limbus (Bracken or Chandler smooth forceps, Westcott scissors) (Fig. 30.1). Note: Take caution to avoid the superior rectus muscle. b. Fashion a thin conjunctival flap down to the limbus, freeing the conjunctiva from subjacent adhesions to Tenon capsule. Have assistant elevate flap while adhesions are lysed with sharp and blunt dissection (smooth forceps, Westcott scissors) (Fig. 30.2). Figure 30.2 Figure 30.3 c. Carefully free remaining adhesions anteriorly using an iris spatula, cellulose sponge, or the back of a scalpel (#15 Bard-Parker blade) (Fig. 30.3). i. Do not buttonhole conjunctiva. ii. Hold flap back with moistened cellulose sponges to avoid trauma to the conjunctiva. iii. Ascertain the anterior extent of the dissection by viewing the iris spatula or scissors blades through the flap (the flap should be dissected well up onto the limbus to avoid placing the sclerostomy too posteriorly). 7. Always keep the conjunctival flap moist with balanced salt solution (BSS). 8. Perform meticulous hemostasis (monopolar microdiathermy). Figure 30.4 9. Remove residual Tenon capsule from the episclera (0.12 mm forceps, Westcott scissors). a. To avoid bleeding, do not cut too close to the episclera. b. Superiorly, cut Tenon off parallel to conjunctival incision (Fig. 30.4). 10. Use calipers to measure width of scleral flap (flap may be rectangular or triangular with an ~3–4 mm base and 3–4 mm posterior extent). 11. Outline edges of scleral flap with microdiathermy. Figure 30.5 12. Make a partial-thickness scleral groove incision (approximately one half to two thirds) over the diathermy outline extending anteriorly to the conjunctival flap (Beaver #57 or Grieshaber #681.01) (Fig. 30.5). Figure 30.6 13. Perform a lamellar dissection of the scleral flap with a scarifier (Fig. 30.6). a. Flap should b ~50% deep. b. Apply counter traction with 0.12 mm or Pierse forceps to facilitate dissection. c. Remain in plane of dissection. d. Extend anteriorly over the limbus to the level of the conjunctival insertion. Optional: Apply mitomycin C (MMC) 0.2 to 0.5 mg/ml or 5-flurouracil 50 mg/ml soaked in a sponge and placed over the scleral dissection area for 1–5 minutes, depending on the desired effect to prevent postoperative fibrosis. Irrigate MMC off eye using BSS. 14. Cauterize planned entry site. Figure 30.7 15. Perform paracentesis through clear cornea just inside the limbus in a quadrant neighboring the filter site with a Wheeler or similar microsurgical knife (see Chapter 7). Note the surrounding landmarks to relocate site at end of case (Fig. 30.7). Note: Temporal placement of paracentesis may facilitate office-based manipulation postoperatively, if necessary. 16. Verify the patency of the paracentesis with a 30 gauge cannula on a syringe. Figure 30.8 17. Enter the anterior chamber under the scleral flap with a microsurgical knife as anteriorly as possible (Fig. 30.8). 18. Extend the entry site horizontally for ~2 mm. Figure 30.9 19. Perform sclerectomy with Kelly Descemet punch (Fig. 30.9). a. Hold the posterior lip of the wound with 0.12 mm forceps to facilitate placing the punch. b. The sclerostomy should be ~2–3 mm long and 1–2 mm wide, with its posterior extent at the level of the scleral spur. c. Alternatively, the trabeculectomy block may be removed in one piece with a microsurgical knife (e.g., Beaver #75M) and Vannas scissors. 20. Cauterize the posterior lip of sclerostomy to expand the opening and prevent bleeding (microdiathermy). Figure 30.10 21. Perform a broad, basal iridectomy (Jeweler’s forceps, Vannas or DeWecker scissors) (Fig. 30.10). 22. Secure the scleral flap with two interrupted 10–0 nylon sutures tied loosely at corners and bury knots (add additional sutures and/or tie more tightly if less filtration is desired). Optional: Postoperatively, indicate in chart which sutures are tight: (e.g., 1 is tightest; 4 loosest). 23. Reposition conjunctival flap. 24. Remove bridle suture or corneal traction suture. Figure 30.11 25. Suture conjunctival flap with either (Fig. 30.11): a. Interrupted 10–0 nylon sutures tied with a 2–1-1 surgeon’s knot. Figure 30.12 26. Check patency of sclerostomy site and security of conjunctival closure by irrigating BSS through the previously placed paracentesis (Fig. 30.12). a. Conjunctival bleb should form and anterior chamber should reform. b. Place 2% fluorescein solution over the suture line and bleb to check for leaks and add additional sutures as necessary. c. If a buttonhole is noted, close with an interrupted or mattress 10–0 nylon suture with a vascular needle. d. Paracentesis site usually does not need to be sutured. 27. Inject subconjunctival Decadron (4–8 mg) 180 degrees away from filter site into the conjunctival fornix. 28. Apply topical antibiotic, steroid ointment, and 1% atro-pine drops. 29. Apply light dressing and shield. Note: The technique of posterior lip sclerectomy is similar to that for trabeculectomy, except that in the former a full-thickness sclerotomy is formed without an overlying scleral flap. 1. Prepare conjunctival flap as in Steps 1 to 9 above. 2. Ensure that the planned sclerectomy site is free of any residual conjunctival adhesions (a site at least 5 mm in length should be prepared). 3. Cauterize limbus at base of conjunctival flap over the planned sclerectomy site (monopolar microdiathermy). 4. Perform paracentesis through clear cornea just inside limbus in quadrant neighboring filter site (Wheeler knife). Figure 30.13 5. Enter the anterior chamber behind the insertion of the conjunctival flap (microsurgical knife) (Fig. 30.13). 6. Extend entry site for ~2–3 mm. Figure 30.14 7. Perform sclerectomy ~2–3 mm long and 1–2 mm wide (Kelly Descemet punch) (Fig. 30.14). a. Hold posterior lip of the wound with 0.12 mm forceps to facilitate placing punch. b. The sclerectomy should be ~1–2 mm wide, its posterior extent at the level of the scleral spur. 8. Cauterize the posterior lip of the sclerectomy to expand the opening and prevent bleeding. 9. Perform broad basal iridectomy (Jeweler’s forceps, Vannas scissors). 10. Reposition and secure the conjunctival flap as in Steps 22 to 30 above. 11. Inject subconjunctival Decadron (4–8 mg) 180 degrees away from filter site into the conjunctival fornix. 12. Apply topical antibiotic, steroid ointment, and 1% atro-pine drops. 13. Apply light dressing and shield. 1. Atropine 1% twice per day until eye is quiet (to prevent posterior synechiae and help maintain deep chamber). 2. Topical antibiotic drops (e.g., moxifloxacin 0.5% [Vigamox, Alcon Laboratories, Inc., Fort Worth, TX, US], gatifloxacin 0.3% [Zymar, Allergan, Inc., Irvine, CA, US]) 4 times per day for 10–14 days. 3. Topical steroid (e.g., prednisolone acetate 1%): from 4 times per day up to every hour, depending upon the degree of inflammation, for ~3 weeks. 4. Optional: Oral steroid (e.g., prednisone 80 mg for 4 days tapering 20 mg/day every 4 days). 5. Keep patient at moderate activity (e.g., bed rest with bathroom privileges, head of bed elevated 30 degrees). 6. Use light patch and Fox shield on first postoperative day, then Fox shield only. May discharge with instructions to wear glasses during the day and Fox shield for protection when sleeping (see Chapter 6.) 7. Avoid aqueous suppressors. Restart carbonic anhydrase inhibitors only if essential for the health of the contralateral eye (since decreased aqueous production can compromise the bleb). 8. Avoid rubbing the eye since minor trauma may precipitate shallowing of the anterior chamber. 9. Apply digital pressure as needed if anterior chamber is deep, IOP too high, and bleb not elevated. 1. Postoperative flat anterior chamber a. Etiology i. Overfiltration or choroidal effusion ii. Wound leak iii. Aqueous diversion syndrome (malignant glaucoma) iv. Decreased aqueous formation secondary to inflammation v. Pupillary block with imperforate or blocked peripheral iridectomy b. Treatment modalities for postoperative flat chamber secondary to overfiltration or choroidal effusion i. Medical treatment I. Vigorous cycloplegia (e.g., cyclopentolate 1% plus phenylephrine 10% every 15 minutes for 2 hours, then 4 times per day and atropine 1% 4 times per day). II. Keep patient at relative rest. III. Keep head of bed at 30 degrees or have patient sit to decrease gravitational filtration. IV. Oral and topical steroids if choroidal effusion appears inflammatory in origin. ii. Pressure patch to decrease filtration. iii. Tamponade filter with glaucoma shell or large soft contact lens. iv. If patient has Seidel-positive wound leak, one or several of the following may be used: I. Torpedo pressure patch. II. Glaucoma shell tamponade or large oversized soft contact lens. III. Medical treatment. A. Decreasing or discontinuing steroids may facilitate wound healing. B. β-blockers (e.g., timolol maleate 0.5%) and carbonic anhydrase inhibitors decrease aqueous flow through the wound gape and may hasten healing. IV. Resuture for large leaks or if other modalities are ineffective. v. If a flat chamber with choroidal effusions persists for 5 days, perform a choroidal tap with reformation of anterior chamber (see Chapter 34). 2. Hyphema. 3. Failure to filter. a. Sutures too tight. Treatment: cut sutures with laser. b. Encapsulated bleb. Treatment: bleb needling. c. Uveal tissue incarceration into sclerostomy. Treatment: laser or surgical revision. 4. Hypotony. 5. Bleb infection. 6. Cataract formation. 7. Corneal endothelial damage. See Chapter 3. 1. The preoperative management of IOP and changes to consider in the patient’s preoperative medical regimen are described in the Trabeculectomy/Posterior Lip Sclerectomy section at the beginning of this chapter. 2. Pupil management. a. If IOP allows, discontinue pilocarpine 24 hours or more preoperatively. c. Optional: If possible, consider discontinuing prostaglandin analog medications 1 week preoperatively or switch to an α-agonist (i.e., brimonidine tartrate 0.1% [Alphagan P] Allergan, Inc.). d. Dilate pupil. i. Cyclopentolate 1%, tropicamide 1%, and phenylephrine 2.5% every 15 minutes starting 1 hour before surgery. ii. Optional: Topical nonsteroidal anti-inflammatory agent (e.g., flurbiprofen 0.03% [Ocufen, Allergan, Inc.],) every 30 minutes starting 2 hours before surgery to minimize intraoperative miosis. 3. The eye should be as quiet as possible preoperatively to enhance the prognosis for successful filtration. a. Optional: Steroid drop 4 times per day to every hour 1 week preoperatively to decrease postoperative inflammation. b. Optional: Oral steroids (e.g., prednisone 80 mg), starting 1 day preoperatively.
Glaucoma Filtration Procedures
 Trabeculectomy/Posterior Lip Sclerectomy
Trabeculectomy/Posterior Lip Sclerectomy
Indications
Preoperative Procedure
Instrumentation
 Lid speculum (e.g., Lieberman)
Lid speculum (e.g., Lieberman)
 Sutures (4–0 silk or 7–0 Vicryl braided, 10–0 nylon or 10–0 Vicryl monofilament)
Sutures (4–0 silk or 7–0 Vicryl braided, 10–0 nylon or 10–0 Vicryl monofilament)
 Kalt needle holder
Kalt needle holder
 Elschnig/tissue forceps
Elschnig/tissue forceps
 3 ml syringe with 30 gauge irrigating cannula
3 ml syringe with 30 gauge irrigating cannula
 Smooth forceps (Chandler or Bracken)
Smooth forceps (Chandler or Bracken)
 Cautery (microdiathermy)
Cautery (microdiathermy)
 Westcott scissors
Westcott scissors
 Iris spatula
Iris spatula
 Castroviejo calipers
Castroviejo calipers
 Scalpel (e.g., #15 Bard-Parker blade)
Scalpel (e.g., #15 Bard-Parker blade)
 Cellulose sponges
Cellulose sponges
 Fine tissue forceps (e.g., 0.12 mm Castroviejo, Pierse)
Fine tissue forceps (e.g., 0.12 mm Castroviejo, Pierse)
 Microsurgical knife (e.g., Beaver #75M, Superblade)
Microsurgical knife (e.g., Beaver #75M, Superblade)
 Scarifier (e.g., Grieshaber #681.01, Beaver #57)
Scarifier (e.g., Grieshaber #681.01, Beaver #57)
 Wheeler or 15-degree microsurgical knife
Wheeler or 15-degree microsurgical knife
 Kelly Descemet membrane punch
Kelly Descemet membrane punch
 Jeweler’s forceps
Jeweler’s forceps
 Vannas scissors
Vannas scissors
 DeWecker scissors
DeWecker scissors
 Tying forceps
Tying forceps
 Needle holder
Needle holder
Operative Procedure
Trabeculectomy


Posterior Lip Sclerectomy (Full-Thickness Filter)
Postoperative Procedure
Complications
 Combined Trabeculectomy, Extracapsular Cataract Extraction, Posterior Chamber Intraocular Lens
Combined Trabeculectomy, Extracapsular Cataract Extraction, Posterior Chamber Intraocular Lens
Indications
 Visually significant cataract in selected patients with moderately severe glaucoma (requiring multiple medications).
Visually significant cataract in selected patients with moderately severe glaucoma (requiring multiple medications).
 Selected patients with cataract and glaucoma requiring filtration surgery for pressure control. If the patient has advanced glaucoma that is poorly controlled, however, a staged procedure filter followed by cataract extraction may have a better prognosis for long-term adequate filtration.
Selected patients with cataract and glaucoma requiring filtration surgery for pressure control. If the patient has advanced glaucoma that is poorly controlled, however, a staged procedure filter followed by cataract extraction may have a better prognosis for long-term adequate filtration.
 Visually significant cataract in a glaucoma patient in whom a transient postoperative pressure rise may be damaging to the optic disc.
Visually significant cataract in a glaucoma patient in whom a transient postoperative pressure rise may be damaging to the optic disc.
Preoperative Procedure
Instrumentation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


