3
Glaucoma
Alex V. Levin and Anya A. Trumler 
PRIMARY CONGENITAL OR INFANTILE GLAUCOMA
Glaucoma diagnosed within the first four years of life and not associated with other findings of anterior segment dysgenesis. When present at birth, it is called congenital glaucoma Characteristic findings include buphthalmos, corneal enlargement, Haab striae (breaks in Descemet’s membrane), increasing axial length, anterior iris insertion on gonioscopy, and corneal edema.
Epidemiology and Etiology
 The incidence of primary congenital or infantile glaucoma varies in different populations of the world with a reported incidence of 1 in 10,000 in the United States. It has a much higher incidence in Saudi Arabia and Gypsies of Romania (one in 2500 and one in 1250, respectively), with both populations having a higher rate of consanguinity.
The incidence of primary congenital or infantile glaucoma varies in different populations of the world with a reported incidence of 1 in 10,000 in the United States. It has a much higher incidence in Saudi Arabia and Gypsies of Romania (one in 2500 and one in 1250, respectively), with both populations having a higher rate of consanguinity.
 Most commonly, mutations in the CYP1B1 (2p21) gene, which encodes a cytochrome P450 protein, are the cause. Two other genes and at least one other locus have been identified. In the Arabic and Gypsy population, a homozygous mutation in CYP1B1 has been found in more than 94% of cases, suggesting an autosomal recessive inheritance. In isolated cases, the frequency of CYP1B1 mutation decreases to 10% to 15%.
Most commonly, mutations in the CYP1B1 (2p21) gene, which encodes a cytochrome P450 protein, are the cause. Two other genes and at least one other locus have been identified. In the Arabic and Gypsy population, a homozygous mutation in CYP1B1 has been found in more than 94% of cases, suggesting an autosomal recessive inheritance. In isolated cases, the frequency of CYP1B1 mutation decreases to 10% to 15%.
 The pathogenesis of primary congenital or infantile glaucoma remains elusive. The theory of an imperforate membrane (Barkan’s membrane) over the trabecular meshwork is controversial. The patients clearly have a goniodysgenesis, which likely represents a failure of complete neural crest differentiation, resulting in impaired aqueous outflow. Clinically, the angle is characterized on gonioscopy as a high flat or patchy high insertion with absence of the angle recess and iris inserting directly on the trabecular meshwork (Fig. 3-1).
The pathogenesis of primary congenital or infantile glaucoma remains elusive. The theory of an imperforate membrane (Barkan’s membrane) over the trabecular meshwork is controversial. The patients clearly have a goniodysgenesis, which likely represents a failure of complete neural crest differentiation, resulting in impaired aqueous outflow. Clinically, the angle is characterized on gonioscopy as a high flat or patchy high insertion with absence of the angle recess and iris inserting directly on the trabecular meshwork (Fig. 3-1).
History
 Primary congenital or infantile glaucoma is bilateral in 75% of cases, which can create a delay in diagnosis because parents may simply believe their child has “beautiful big eyes.”
Primary congenital or infantile glaucoma is bilateral in 75% of cases, which can create a delay in diagnosis because parents may simply believe their child has “beautiful big eyes.”
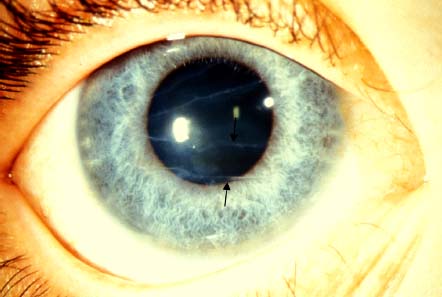
 The classic symptom triad is photophobia, epiphora, and blepharospasm. Buphthalmic eyes with corneal stromal or epithelial edema (Fig. 3-2) is often the presenting sign.
The classic symptom triad is photophobia, epiphora, and blepharospasm. Buphthalmic eyes with corneal stromal or epithelial edema (Fig. 3-2) is often the presenting sign.
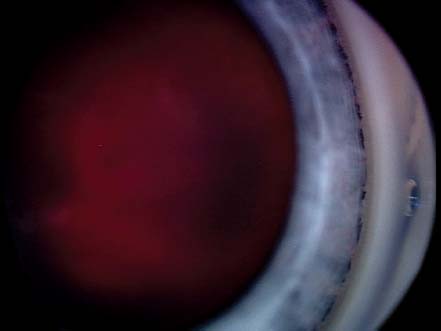
 Elevated IOP causes stretching of the cornea with resultant breaks in Descemet’s membrane, called Haab striae (Fig. 3-3). The stretching of the anterior segment also gives the sclera a blue appearance because of the underlying hue of the uvea.
Elevated IOP causes stretching of the cornea with resultant breaks in Descemet’s membrane, called Haab striae (Fig. 3-3). The stretching of the anterior segment also gives the sclera a blue appearance because of the underlying hue of the uvea.
Signs
 Characteristic findings include increased IOP, optic nerve cupping, corneal enlargement, Haab striae, increasing axial length, and gonioscopy findings (see Diagnostic Evaluation section).
Characteristic findings include increased IOP, optic nerve cupping, corneal enlargement, Haab striae, increasing axial length, and gonioscopy findings (see Diagnostic Evaluation section).
Differential Diagnosis
 Congenital hereditary endothelial dystrophy (CHED)
Congenital hereditary endothelial dystrophy (CHED)
 Congenital hereditary stromal dystrophy (CHSD)
Congenital hereditary stromal dystrophy (CHSD)
 Mucopolysaccharidosis
Mucopolysaccharidosis
 Sclerocornea or Peters’ anomaly
Sclerocornea or Peters’ anomaly
 Keratitis
Keratitis
 Forceps birth trauma
Forceps birth trauma
 Megalocornea
Megalocornea
 Contralateral microphthalmia
Contralateral microphthalmia
 Nasolacrimal duct obstruction
Nasolacrimal duct obstruction
Diagnostic Evaluation
 A patient with corneal clouding, increased corneal diameter, and optic nerve cupping should raise the suspicion for primary congenital or infantile glaucoma and prompt further evaluation with an examination under anesthesia, including biomicroscopy, pachymetry, corneal diameter measurement, gonioscopy, refraction, axial length measurement, and (if possible) optic nerve photography.
A patient with corneal clouding, increased corneal diameter, and optic nerve cupping should raise the suspicion for primary congenital or infantile glaucoma and prompt further evaluation with an examination under anesthesia, including biomicroscopy, pachymetry, corneal diameter measurement, gonioscopy, refraction, axial length measurement, and (if possible) optic nerve photography.
 When measuring intraocular pressure (IOP) under anesthesia, attention should be paid regarding the type of anesthetic agent used. Whereas ketamine increases IOP measurements, halothane significantly lowers IOP, as do other anesthetic agents but to a lesser extent.
When measuring intraocular pressure (IOP) under anesthesia, attention should be paid regarding the type of anesthetic agent used. Whereas ketamine increases IOP measurements, halothane significantly lowers IOP, as do other anesthetic agents but to a lesser extent.
 Corneal hysteresis should be taken into account because corneal edema falsely lowers the IOP measurements. Asymmetry of IOP of 5 mm Hg is also an important indication of an abnormality.
Corneal hysteresis should be taken into account because corneal edema falsely lowers the IOP measurements. Asymmetry of IOP of 5 mm Hg is also an important indication of an abnormality.
 The normal corneal diameter in an infant younger than 1 year of age is 11 mm, with a corneal diameter greater than 12 mm, asymmetry between the eyes, and significant progression over time all being suggestive of primary congenital or infantile glaucoma.
The normal corneal diameter in an infant younger than 1 year of age is 11 mm, with a corneal diameter greater than 12 mm, asymmetry between the eyes, and significant progression over time all being suggestive of primary congenital or infantile glaucoma.
 Retinoscopy and axial length measurement using immersion A-scan provides objective measurements to suggest increased axial length. The mean axial length at birth is 17 mm and increases to 20 mm by 1 year of age.
Retinoscopy and axial length measurement using immersion A-scan provides objective measurements to suggest increased axial length. The mean axial length at birth is 17 mm and increases to 20 mm by 1 year of age.
Treatment and Prognosis
 Medical management with antiglaucoma medications in primary congenital or infantile glaucoma is used as a temporizing agent, with definitive treatment being surgical.
Medical management with antiglaucoma medications in primary congenital or infantile glaucoma is used as a temporizing agent, with definitive treatment being surgical.
 Antiglaucoma medications, including carbonic anhydrase inhibitors (both topical and oral), low-dose beta-blockers, and prostaglandins, may be used to clear the cornea for surgical intervention. Brimonidine should not be used in infants younger than the age of 1 year because there is a risk of potentially life-threatening apnea, hypotension, bradycardia, and hypothermia.
Antiglaucoma medications, including carbonic anhydrase inhibitors (both topical and oral), low-dose beta-blockers, and prostaglandins, may be used to clear the cornea for surgical intervention. Brimonidine should not be used in infants younger than the age of 1 year because there is a risk of potentially life-threatening apnea, hypotension, bradycardia, and hypothermia.
 The primary procedure of choice in primary congenital or infantile glaucoma is goniotomy or trabeculotomy depending on the preference of the surgeon and adequate visualization of anterior chamber angle that is needed for goniotomy. Both have reported short-term success rates of 60% to 90%. In one epidemiologic study, goniotomy offered a long-term cure in only 48.7% of patients. In patients who have failed goniotomy or trabeculotomy, secondary surgery may include goniosurgery on the remaining angle or trabeculectomy or glaucoma drainage device.
The primary procedure of choice in primary congenital or infantile glaucoma is goniotomy or trabeculotomy depending on the preference of the surgeon and adequate visualization of anterior chamber angle that is needed for goniotomy. Both have reported short-term success rates of 60% to 90%. In one epidemiologic study, goniotomy offered a long-term cure in only 48.7% of patients. In patients who have failed goniotomy or trabeculotomy, secondary surgery may include goniosurgery on the remaining angle or trabeculectomy or glaucoma drainage device.
 The goal of primary congenital or infantile glaucoma treatment is more than achieving a normal IOP but more importantly attaining and maintaining normal visual function. Aggressive treatment of refractive error, amblyopia, and visually significant optical opacities are an important component to the infant’s care. Lifelong follow-up of these patients is needed to monitor for glaucoma progression. Optic nerve cupping in infants is reversible and is a hallmark of successful glaucoma management. The most common cause of visual loss is amblyopia.
The goal of primary congenital or infantile glaucoma treatment is more than achieving a normal IOP but more importantly attaining and maintaining normal visual function. Aggressive treatment of refractive error, amblyopia, and visually significant optical opacities are an important component to the infant’s care. Lifelong follow-up of these patients is needed to monitor for glaucoma progression. Optic nerve cupping in infants is reversible and is a hallmark of successful glaucoma management. The most common cause of visual loss is amblyopia.
REFERENCES
Bejjani BA, Lewis RA, Tomey KF, et al. Mutations in CYP1B1, the gene for cytochrome P4501B1, are the predominant cause of primary congenital glaucoma in Saudi Arabia. Am J Hum Genet. 1998;62:325–333.
Curry SM, Daou AG, Hermanns P, et al. Cytochrome P4501B1 mutations cause only part of primary congenital glaucoma in Ecuador. Ophthalmic Genet. 2004;25:3–9.
Debnath SC, Teichmann KD, Salamah K. Trabeculectomy versus trabeculotomy in congenital glaucoma. Br J Ophthalmol. 1989;73:608–611.
Gencik A. Epidemiology and genetics of primary congenital glaucoma in Slovakia. Description of a form of primary congenital glaucoma in gypsies with autosomal-recessive inheritance and complete penetrance. Dev Ophthalmol. 1989;16:76–115.
Plasilova M, Stoilov I, Sarfarazi M, et al. Identification of a single ancestral CYP1B1 mutation in Slovak Gypsies (Roms) affected with primary congenital glaucoma. J Med Genet. 1999;36:290–294.
Taylor RH, Ainsworth JR, Evans AR, et al. The epidemiology of pediatric glaucoma: the Toronto experience. J AAPOS. 1999;3:308–315.
FIGURE 3-1. Gonioscopic view of a child with infantile glaucoma angle showing patches of high iris insertion (arrows).
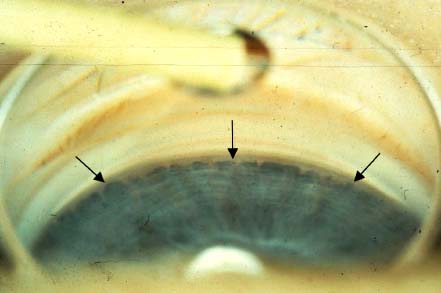
FIGURE 3-2. Buphthalmos and corneal clouding of the right eye. Miosis in the right eye is caused by the use of pilocarpine.

FIGURE 3-3. Haab striae, which are breaks in Descemet’s membrane, are delineated by the appearance of two scrolled back edges (arrows denote the bottom Haab stria; there is also one more superiorly).
JUVENILE OPEN-ANGLE GLAUCOMA
Juvenile open-angle glaucoma (JOAG) is a form of open-angle primary glaucoma unassociated with ocular malformations, with an age of onset from age 4 to 40 years old. JOAG generally has a more aggressive course than the later onset adult primary open-angle glaucoma.
Epidemiology and Etiology
 The incidence of JOAG is 1 per 50,000 cases of all glaucoma. It has autosomal dominant inheritance with variable expression and penetrance. The most commonly mutated gene is the myocilin gene (MYOC) on chromosome 1q21-q31 (termed GLC1A). Myocilin is a glycoprotein that is expressed in the trabecular meshwork, with its function unknown. Mutations in the CYP1B1 gene on chromosome 2p21 have been associated with autosomal recessive inheritance of juvenile onset glaucoma. Patients with a mutation in CYP1B1 in addition to MYOC have a more severe phenotype than those with MYOC mutation alone. The pathophysiology of JOAG is unknown but is thought to be impaired aqueous outflow through the trabecular meshwork. There are usually no abnormalities on gonioscopy in affected patients, although there are histologic reports of thickening of the trabecular meshwork outflow system and clinical reports of increased iris processes (“pectinate ligaments”) crossing the trabecular meshwork.
The incidence of JOAG is 1 per 50,000 cases of all glaucoma. It has autosomal dominant inheritance with variable expression and penetrance. The most commonly mutated gene is the myocilin gene (MYOC) on chromosome 1q21-q31 (termed GLC1A). Myocilin is a glycoprotein that is expressed in the trabecular meshwork, with its function unknown. Mutations in the CYP1B1 gene on chromosome 2p21 have been associated with autosomal recessive inheritance of juvenile onset glaucoma. Patients with a mutation in CYP1B1 in addition to MYOC have a more severe phenotype than those with MYOC mutation alone. The pathophysiology of JOAG is unknown but is thought to be impaired aqueous outflow through the trabecular meshwork. There are usually no abnormalities on gonioscopy in affected patients, although there are histologic reports of thickening of the trabecular meshwork outflow system and clinical reports of increased iris processes (“pectinate ligaments”) crossing the trabecular meshwork.
 Genetic studies of large families (e.g., the one shown in .2) demonstrated that defects or mutations in the myocilin gene are a cause of JOAG. Most cases of JOAG that have a strong family history of disease are associated with defects in the myocilin gene (MYOC). Myocilin associated glaucoma is inherited as an autosomal dominant trait. That is, patients carrying a myocilin mutation that causes JOAG have a 50% chance of passing the gene (and high risk for glaucoma) to their children. Several specific defects or mutations in MYOC that cause JOAG have been identified. Some patients have the typical clinical features of JOAG but do not have a family history of disease. MYOC has a less important role in these sporadic cases of JOAG.
Genetic studies of large families (e.g., the one shown in .2) demonstrated that defects or mutations in the myocilin gene are a cause of JOAG. Most cases of JOAG that have a strong family history of disease are associated with defects in the myocilin gene (MYOC). Myocilin associated glaucoma is inherited as an autosomal dominant trait. That is, patients carrying a myocilin mutation that causes JOAG have a 50% chance of passing the gene (and high risk for glaucoma) to their children. Several specific defects or mutations in MYOC that cause JOAG have been identified. Some patients have the typical clinical features of JOAG but do not have a family history of disease. MYOC has a less important role in these sporadic cases of JOAG.
History
 Patients are usually asymptomatic. Often, the disorder is noted as an incidental finding during routine examination.
Patients are usually asymptomatic. Often, the disorder is noted as an incidental finding during routine examination.
 Because it is most commonly an autosomal dominant disorder, all family members of affected individuals should have a comprehensive examination.
Because it is most commonly an autosomal dominant disorder, all family members of affected individuals should have a comprehensive examination.
Signs
 Complete anterior segment examination is important to assess for secondary causes of glaucoma. IOP measurement with routine ophthalmic examinations helps in identifying new cases.
Complete anterior segment examination is important to assess for secondary causes of glaucoma. IOP measurement with routine ophthalmic examinations helps in identifying new cases.
 At-risk patients should be examined at least twice yearly.
At-risk patients should be examined at least twice yearly.
 Patients with increased cup-to-disc ratio or asymmetry should undergo IOP measurements, gonioscopy, pachymetry, visual field testing, optical coherence tomography, and optic nerve photos with serial follow-up.
Patients with increased cup-to-disc ratio or asymmetry should undergo IOP measurements, gonioscopy, pachymetry, visual field testing, optical coherence tomography, and optic nerve photos with serial follow-up.
Differential Diagnosis
 Glaucoma secondary to uveitis
Glaucoma secondary to uveitis
 Glaucoma associated with anterior segment dysgenesis
Glaucoma associated with anterior segment dysgenesis
 Steroid-induced glaucoma
Steroid-induced glaucoma
 Traumatic (e.g., angle recession) glaucoma
Traumatic (e.g., angle recession) glaucoma
 Physiologic cupping
Physiologic cupping
Diagnostic Evaluation
 At-risk children based on family history (one affected parent or sibling) should have IOP measurements serially even if sedation or anesthesia is required. Evaluation should include a comprehensive ophthalmic examination, including, vision, refraction, slit-lamp examination, pachymetry, gonioscopy, and ophthalmoscopy. Gonioscopy is not diagnostic but is useful in evaluating for secondary causes of glaucoma. The presence of increased numbers of iris processes may or may not represent an indicator of risk for JOAG.
At-risk children based on family history (one affected parent or sibling) should have IOP measurements serially even if sedation or anesthesia is required. Evaluation should include a comprehensive ophthalmic examination, including, vision, refraction, slit-lamp examination, pachymetry, gonioscopy, and ophthalmoscopy. Gonioscopy is not diagnostic but is useful in evaluating for secondary causes of glaucoma. The presence of increased numbers of iris processes may or may not represent an indicator of risk for JOAG.
 Patients with the clinical appearance of glaucomatous optic neuropathy with normal IOP on isolated visits should also undergo diurnal curve testing to assess pressure variation as well as maximum daily pressure.
Patients with the clinical appearance of glaucomatous optic neuropathy with normal IOP on isolated visits should also undergo diurnal curve testing to assess pressure variation as well as maximum daily pressure.
 Automated visual field testing in young patients can be difficult, with Goldman visual field testing often being a better assessment tool.
Automated visual field testing in young patients can be difficult, with Goldman visual field testing often being a better assessment tool.
 Optical coherence tomography currently has limited available normative data for children, but asymmetry between the two eyes and changes over time can be used as indicators of abnormality. Optic nerve photography is useful in documenting and monitoring change in the appearance of the optic nerves.
Optical coherence tomography currently has limited available normative data for children, but asymmetry between the two eyes and changes over time can be used as indicators of abnormality. Optic nerve photography is useful in documenting and monitoring change in the appearance of the optic nerves.
 Physiologic cupping, also an autosomal dominant condition, must be considered (Fig. 3-4) but is difficult to distinguish from JOAG other than the absence of elevated IOP, change over time, or visual field deficits. Physiologic cups tend to have very distinct sharp borders and may be eccentric within the disc. Patients’ parents should be examined for similar findings and, if present, their IOP should be checked as well. It may take several visits over months or years to be confident that there is no progression and thus no JOAG.
Physiologic cupping, also an autosomal dominant condition, must be considered (Fig. 3-4) but is difficult to distinguish from JOAG other than the absence of elevated IOP, change over time, or visual field deficits. Physiologic cups tend to have very distinct sharp borders and may be eccentric within the disc. Patients’ parents should be examined for similar findings and, if present, their IOP should be checked as well. It may take several visits over months or years to be confident that there is no progression and thus no JOAG.
Treatment and Prognosis
 JOAG tends to be more aggressive, more resistant to medical therapy, and associated with more severe visual impairment.
JOAG tends to be more aggressive, more resistant to medical therapy, and associated with more severe visual impairment.
 The use of topical antiglaucoma medications is the first line of treatment followed by oral carbonic anhydrase inhibitors.
The use of topical antiglaucoma medications is the first line of treatment followed by oral carbonic anhydrase inhibitors.
 JOAG patients require close follow-up until maintenance of an acceptable IOP is achieved.
JOAG patients require close follow-up until maintenance of an acceptable IOP is achieved.
 Most cases over the long term are progressive and require surgical intervention.
Most cases over the long term are progressive and require surgical intervention.
 Some evidence indicates that goniotomy and trabeculotomy can be successful. More traditionally, trabeculectomy or glaucoma drainage device surgery is the first surgical intervention. Trabeculectomy has similar success rates to those done on patients with primary open-angle glaucoma.
Some evidence indicates that goniotomy and trabeculotomy can be successful. More traditionally, trabeculectomy or glaucoma drainage device surgery is the first surgical intervention. Trabeculectomy has similar success rates to those done on patients with primary open-angle glaucoma.
REFERENCES
Jacobi PC, Dietlein TS, Krieglstein GK. Primary trabeculectomy in young adults: long-term clinical results and factors influencing the outcome. Ophthalmic Surg Lasers. 1999;30:637–646.
Park SC, Kee C. Large diurnal variation of intraocular pressure despite maximal medical treatment in juvenile open angle glaucoma. J Glaucoma. 2007;16:164–168.
Stoilova D, Child A, Brice G, et al. Novel TIGR/MYOC mutations in families with juvenile onset primary open angle glaucoma. J Med Genet. 1998;35:989–992.
Vincent AL, Billingsley G, Buys Y, et al. Digenic inheritance of early-onset glaucoma: CYP1B1, a potential modifier gene. Am J Hum Genet. 2002;70:448–460.
Yeung HH, Walton DS. Goniotomy for juvenile open-angle glaucoma. J Glaucoma. 2010;19:1–4.
FIGURE 3-4. Physiologic cup. Note the sharp margin to the cup and scooped-out appearance. The vessels disappear as they turn posteriorly at the margin of the cup. The father, who did not have glaucoma, has a similar appearance to his optic nerve heads.

APHAKIC GLAUCOMA
Aphakic glaucoma is glaucoma that develops in an eye that is aphakic.
Epidemiology and Etiology
 Aphakic glaucoma is the most common complication of congenital cataract surgery with an incidence up to 32%. Theories as to the etiology include abnormal development of the anterior chamber angle, genetic predisposition, barotrauma incurred during surgery, decreased structural support to the drainage angle from aphakia, vitreous affecting angle structures, and release of chemical mediators that affect aqueous drainage.
Aphakic glaucoma is the most common complication of congenital cataract surgery with an incidence up to 32%. Theories as to the etiology include abnormal development of the anterior chamber angle, genetic predisposition, barotrauma incurred during surgery, decreased structural support to the drainage angle from aphakia, vitreous affecting angle structures, and release of chemical mediators that affect aqueous drainage.
 Despite advances in cataract surgery, it is clear that the prevention of glaucoma after cataract surgery has not been well understood. Even with the use of intraocular lens implantation in the pediatric population, the incidence of glaucoma appears to be unchanged.
Despite advances in cataract surgery, it is clear that the prevention of glaucoma after cataract surgery has not been well understood. Even with the use of intraocular lens implantation in the pediatric population, the incidence of glaucoma appears to be unchanged.
 Factors associated with a higher risk of development of glaucoma are surgery within the first year of life, corneal diameter less than 10 mm, presence of other ocular anomalies, retained lens material, nuclear cataract, and eyes that require secondary surgeries.
Factors associated with a higher risk of development of glaucoma are surgery within the first year of life, corneal diameter less than 10 mm, presence of other ocular anomalies, retained lens material, nuclear cataract, and eyes that require secondary surgeries.
History
 Similar to congenital infantile glaucoma, the symptom triad of photophobia, epiphora, and blepharospasm is often seen in those who develop aphakic glaucoma before age 3 years.
Similar to congenital infantile glaucoma, the symptom triad of photophobia, epiphora, and blepharospasm is often seen in those who develop aphakic glaucoma before age 3 years.
 Most patients are asymptomatic.
Most patients are asymptomatic.
 The onset of glaucoma may occur early after surgery or later in childhood, with the average age to onset approximately 4 to 8 years after surgery.
The onset of glaucoma may occur early after surgery or later in childhood, with the average age to onset approximately 4 to 8 years after surgery.
 Routine lifelong screening of all aphakic patients is important for the early diagnosis of glaucoma.
Routine lifelong screening of all aphakic patients is important for the early diagnosis of glaucoma.
Signs
 Early signs of glaucoma include a decrease in the amount of aphakic refraction (rapid loss of hyperopia caused by globe elongation), corneal clouding, and increased corneal diameter in patients who develop glaucoma generally before age 3 years old.
Early signs of glaucoma include a decrease in the amount of aphakic refraction (rapid loss of hyperopia caused by globe elongation), corneal clouding, and increased corneal diameter in patients who develop glaucoma generally before age 3 years old.
 Most patients are asymptomatic, and elevated IOP and optic nerve cupping are found on screening examination.
Most patients are asymptomatic, and elevated IOP and optic nerve cupping are found on screening examination.
Differential Diagnosis
 Primary infantile glaucoma
Primary infantile glaucoma
 Anterior segment dysgenesis
Anterior segment dysgenesis
 Uveitic glaucoma
Uveitic glaucoma
 Traumatic glaucoma
Traumatic glaucoma
Diagnostic Evaluation
 Pediatric patients who are left aphakic after cataract surgery should be examined for glaucoma on a regular basis, certainly no less than annually. When patients are too young for IOP measurement or optic nerve evaluation, an examination under anesthesia or sedation may be needed.
Pediatric patients who are left aphakic after cataract surgery should be examined for glaucoma on a regular basis, certainly no less than annually. When patients are too young for IOP measurement or optic nerve evaluation, an examination under anesthesia or sedation may be needed.
 Early signs of glaucoma include a decrease in the amount of aphakic refraction, corneal clouding, increased corneal diameter in young patients, and optic nerve cupping. The presence of peripheral or midperipheral anterior synechia or posterior synechia with iris bombe speaks to an inflammatory component.
Early signs of glaucoma include a decrease in the amount of aphakic refraction, corneal clouding, increased corneal diameter in young patients, and optic nerve cupping. The presence of peripheral or midperipheral anterior synechia or posterior synechia with iris bombe speaks to an inflammatory component.
 Biomicroscopy, corneal diameter measurement, pachymetry (which is often elevated in aphakia and pseudophakia), gonioscopy, axial length measurement, and optic nerve photography are all important components of an examination under anesthesia.
Biomicroscopy, corneal diameter measurement, pachymetry (which is often elevated in aphakia and pseudophakia), gonioscopy, axial length measurement, and optic nerve photography are all important components of an examination under anesthesia.
 Gonioscopy may show an angle configuration similar to that seen in primary infantile glaucoma (Fig. 3-5) or may have peripheral anterior synechia.
Gonioscopy may show an angle configuration similar to that seen in primary infantile glaucoma (Fig. 3-5) or may have peripheral anterior synechia.
 Preoperative evaluation and measurements are useful in monitoring progression in those who require cataract surgery if aphakic or pseudophakic glaucoma later develops.
Preoperative evaluation and measurements are useful in monitoring progression in those who require cataract surgery if aphakic or pseudophakic glaucoma later develops.
Treatment and Prognosis
 The first line of treatment of patients with aphakic glaucoma is one or more antiglaucoma medications, which in many cases prove effective in lowering the IOP.
The first line of treatment of patients with aphakic glaucoma is one or more antiglaucoma medications, which in many cases prove effective in lowering the IOP.
 When topical and oral medications fail, surgery is often successful, with goniotomy or trabeculotomy surgery being effective in approximately 55% of patients.
When topical and oral medications fail, surgery is often successful, with goniotomy or trabeculotomy surgery being effective in approximately 55% of patients.
 If the above procedures fail, then a trabeculectomy or glaucoma drainage device may be implanted. Endoscopic diode cyclophotoabaltion may provide another early option for treatment. Otherwise, cycloablation plays a role in cases of refractive glaucoma.
If the above procedures fail, then a trabeculectomy or glaucoma drainage device may be implanted. Endoscopic diode cyclophotoabaltion may provide another early option for treatment. Otherwise, cycloablation plays a role in cases of refractive glaucoma.
 Early detection and treatment of glaucoma are important in improving the likelihood of preventing optic nerve progression and preserving visual function.
Early detection and treatment of glaucoma are important in improving the likelihood of preventing optic nerve progression and preserving visual function.
 Aggressive treatment of refractive error, amblyopia, and visually significant optical opacities are also vital components of pediatric patients’ eye care.
Aggressive treatment of refractive error, amblyopia, and visually significant optical opacities are also vital components of pediatric patients’ eye care.
REFERENCES
Bothun ED, Guo Y, Christiansen SP, et al. Outcome of angle surgery in children with aphakic glaucoma. J AAPOS. 2010;14:235–239.
Chen TC, Walton DS, Bhatia LS. Aphakic glaucoma after congenital cataract surgery. Arch Ophthalmol. 2004; 122:1819–1825.
Levin AV. Aphakic glaucoma: a never-ending story? Br J Ophthalmol. 2007;91:1574–1575.
FIGURE 3-5. Gonioscopy of the angle in aphakic glaucoma appears similar to infantile glaucoma with patches of high iris insertion. This patient may be a good candidate for goniolytic surgery.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


