1 General
Indications and Contraindications
Risks and Complications: Cardiac and Pulmonary
Risks and Complications: Gastrointestinal
Endoscopy Suite: Facilities and Staff
Preparations for Endoscopy: Informed Consent
Preparations for Endoscopy: Medications (1)
Preparations for Endoscopy: Medications (2)
Checklists Before, During, and After the Examination
Diagnosis and Treatment of Complications (1)
Diagnosis and Treatment of Complications (2)
Diagnosis and Treatment of Complications (3)
Diagnosis and Treatment of Complications (4)
Diagnosis and Treatment of Complications (5)
Endoscopic Technique: Steps in Learning
Endoscopic Technique: Maneuvering the Scope
Endoscopic Technique: Functions
Indications and Contraindications
Upper gastrointestinal endoscopy, known also as upper GI endoscopy or esophagogastroduodenoscopy (EGD), is the method of choice for examining the esophagus, stomach, and duodenum. In one sitting, it permits the gross visual inspection of the upper gastrointestinal tract, the collection of tissue and fluid samples, as well as elective and emergency therapeutic interventions. It can be performed quickly and safely with good patient tolerance and without extensive patient preparations. The requirements in terms of equipment and operator proficiency are relatively modest.
 Indications
Indications
Upper GI endoscopy has a broad range of indications. It is used to confirm or exclude a particular diagnosis in patients with upper gastrointestinal complaints, to monitor the progression of a known disease, and for staging in patients with a systemic disease (Fig. 1.1).
 Contraindications
Contraindications
An absolute contraindication to elective upper GI endoscopy is lack of informed consent from a mentally competent patient. Relative contraindications are organ perforations and states of cardiac or respiratory decompensation (Fig. 1.2).
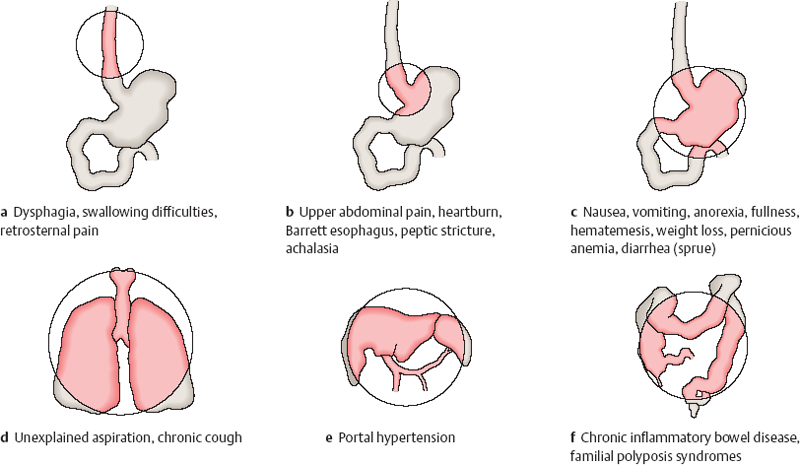
Fig. 1.1 Indications
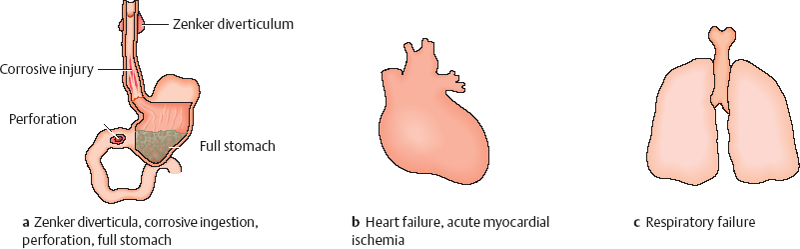
Fig. 1.2 Relative contraindications
Risks and Complications: Cardiac and Pulmonary
The rate of serious complications in upper GI endoscopy is small and is measured in tenths of a percent (Table 1.1). Reports based on larger reviews show that the mortality rate is less than 0.01%.
It should be emphasized that most complications do not involve the gastrointestinal tract itself but consist of respiratory or cardiovascular incidents, especially in sick or sedated patients (Table 1.2).
Complications can result from local anesthesia, sedation, or the endoscopy itself. They consist mainly of respiratory and cardiovascular events, mechanical injuries, hemorrhages, and infections.
| Complication | Complication rate | Percentage of all complications |
|---|---|---|
| Cardiac | 1:2000 | 60% |
| Pulmonary | 1:4000 | 30% |
| Perforation, bleeding | 1:15000 | 9% |
| Infection | 1:50000 | 1% |
|
 Advanced age
Advanced age NYHA class III-IV heart failure
NYHA class III-IV heart failure Grade III-IV aortic stenosis
Grade III-IV aortic stenosis Severe pulmonary disease
Severe pulmonary disease Bleeding tendency (Quick prothrombin < 50 %, thrombopenia < 50 000/μL)
Bleeding tendency (Quick prothrombin < 50 %, thrombopenia < 50 000/μL) Anemia (Hb <8g/dL)
Anemia (Hb <8g/dL) Emergency procedures
Emergency procedures
 Local Anesthesia
Local Anesthesia
Anesthetic throat sprays have the potential to incite an allergic reaction, produce cardiac side effects, and promote aspiration. The overall risk of complications from pharyngeal anesthesia is approximately 1:10 000. The risk of fatal complications is considerably lower.
 Sedation and Analgesia
Sedation and Analgesia
Benzodiazepines. The use of benzodiazepines is often associated with a decrease in arterial oxygen saturation, but this is rarely significant. The risk is increased in older patients, patients with chronic respiratory failure, coronary heart disease, or hepatic insufficiency, and in emergency endoscopy.
The principal risks are a fall in blood pressure and hypoxemia-induced cardiac arrhythmia. Myocardial infarctions during endoscopy are rare. Respiratory complications can range from hypoventilation to apnea. The most common problem is aspiration. Sedation is believed to be the principal risk factor for aspiration pneumonia.
Narcotics. The use of narcotic analgesics, such as Pethidine, can lead to hypotension and bradycardia.
 Cardiac Complications
Cardiac Complications
Approximately 50 % of the complications that occur in upper GI endoscopy are cardiac in nature. They consist of heart rate changes, arrhythmias, and repolarization abnormalities. The mortality rate of cardiac complications ranges from 1:20000 to 1:50 000.
Arrhythmias. The most common arrhythmias are tachycardia and extrasystoles, which usually have no clinical significance and are spontaneously reversible. Bradycardia is observed in fewer than 5 % of patients. Significant tachyarrhythmias are also rare.
Repolarization abnormalities. These occur predominantly in patients with coronary heart disease. They reflect a myocardial ischemia, usually clinically silent, that is caused by arterial hypoxia due to the increased cardiac work load.
 Respiratory Complications
Respiratory Complications
Respiratory complications consist of hypoventilation, apnea, and aspiration, usually in connection with premedication. Their overall incidence is low, however. The mortality rate is less than 1:50 000.
Risks and Complications: Gastrointestinal
 Perforation and Bleeding
Perforation and Bleeding
Although perforation and bleeding from gastroscopy are the complications that patients fear the most, they account for less than 10% of all complications in diagnostic endoscopy.
The most common sites of perforation, in descending order of frequency, are the esophagus, hypopharynx, duodenum, and stomach. Predisposing factors are diverticula, severe cervical spondylosis, and endoscopic interventions such as dilation, prosthesis insertion, and laser therapy (Fig. 1.3). Severe postbiopsy bleeding during or after endoscopy is rare.
 Infection
Infection
The risk of clinically overt infection after upper GI endoscopy is extremely small, but does exist. Bacteremia is a common occurrence, however. Three factors are relevant in the pathogenesis of infection: the transmission of infectious organisms, the nature of the procedure, and patient-associated risks (Table 1.3).
Disease Transmission
The direct transmission of microorganisms from patient to patient by contaminated endoscopes has been described for Salmonellae, mycobacteria, Helicobacter pylori, hepatitis B virus, and other pathogens. The endoscopic transmission of HIV infection has not yet been definitely confirmed.
Bacteremia is not uncommon after endoscopy (up to 5 % of cases) but usually has no clinical significance. The endoscope itself can be a reservoir for pathogenic microorganisms (including pseudomonas). Potential sources of infection are contaminated water bottles and the endoscope channels that are more difficult to access and clean. Meticulous cleaning and disinfection after each endoscopy and before the first endoscopy of the day are essential elements of risk management.
Nature of the Procedure
It is clear that procedures that inflict mucosal injuries are associated with a higher infection risk than a simple, uncomplicated endoscopy. Antibiotic prophylaxis should be used liberally in cases deemed to be at risk.
Patient-Associated Risks
These risks consist mainly of cardiac anomalies, prosthetic valves, and immunosuppression. The regimen shown in Table 1.4 is recommended for general antibiotic prophylaxis but should be tailored to suit individual clinical requirements.
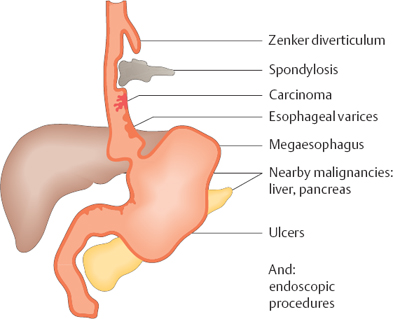
Fig. 1.3 Perforation and bleeding. Predisposing factors
Transmission of infectious organisms
|
Nature of the procedure
|
Patient
|
 From the previously examined patient
From the previously examined patient Endogenous transmission (bacteremia)
Endogenous transmission (bacteremia) Contaminated endoscope
Contaminated endoscope Simple endoscopy
Simple endoscopy Tissue or fluid sampling
Tissue or fluid sampling Polypectomy
Polypectomy Injection
Injection Bougie or balloon dilation, stenting, prosthesis insertion
Bougie or balloon dilation, stenting, prosthesis insertion Cardiac valve defects
Cardiac valve defects Artificial heart valve
Artificial heart valve Indwelling venous catheter, port
Indwelling venous catheter, port Immunosuppression
Immunosuppression Hematological disease
Hematological disease Immune-suppressing drugs
Immune-suppressing drugs HIV infection
HIV infection Advanced liver or kidney disease
Advanced liver or kidney disease Diagnostic endoscopy
|
Interventional endoscopy
|
In patients allergic to penicillin
|
 Ampicillin, 2 g orally 30-60 min before the procedure
Ampicillin, 2 g orally 30-60 min before the procedure Ampicillin, 1.5 g orally 6 hours after the procedure
Ampicillin, 1.5 g orally 6 hours after the procedure Add before the procedure: 80 mg gentamycin i. v. or 2 g cefotaxime i. v.
Add before the procedure: 80 mg gentamycin i. v. or 2 g cefotaxime i. v.  Clindamycin, 600 mg orally 1 hour before the procedure
Clindamycin, 600 mg orally 1 hour before the procedure
Endoscopy Suite: Facilities and Staff
The size, equipment, and organization of the endoscopy suite are determined by the frequency of endoscopic procedures and the requirements that they must satisfy.
 Procedure Room
Procedure Room
Room. The procedure room should be large enough to accommodate all necessary instruments and equipment, the recumbent patient, and at least two other people. The room should have bright lighting that can be dimmed when necessary. Access to fresh air is desirable. Cleaning requirements should be considered during planning and setup of the room. A toilet and recovery area should be easily accessible.
Equipment. The minimum equipment and instruments needed for an endoscopy suite are the endoscope and supply unit, a cleaning area, examination table, sinks, emergency equipment, storage space for drugs, disposables, and accessories, and places for the patient and examiner to sit down.
 Staff
Staff
Assistants. Although an experienced endoscopist can work successfully with inexperienced assistants, specially trained assistants are essential for more complex examinations and for procedures in high-risk patients. An experienced, efficient endoscopy nurse is an invaluable asset to the beginner.
Functions. The functions of the endoscopy nursing staff include setting up the necessary equipment, preparing the patient, assisting the endoscopist in inserting and advancing the instrument, observing the patient, comforting and reassuring the patient during the procedure, assisting with specimen collection, monitoring the patient’s recovery, and cleaning and processing the equipment. The nursing staff should know the basic rules of emergency care in the event that complications arise. Endoscopy team members with a negative hepatitis A or B immune status should be immunized without delay.
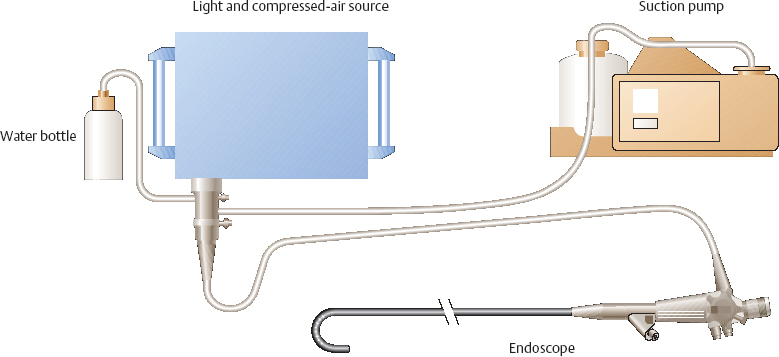
Fig. 1.4 Endoscopy unit
 Endoscopy Unit
Endoscopy Unit
The endoscopy unit in the strict sense consists of the supply unit, the endoscope, and the cleaning area (Fig. 1.4).
Supply Unit
The supply unit consists of a light source, a compressed air pump for delivering air and water, a suction pump, and a video processor (for video endoscopy). These units converge at the supply plug of the endoscope.
Endoscopy Suite: Endoscope
Components of the Endoscope
The endoscope consists of the supply plug, umbilical cord, control head, insertion tube (shaft), and bending section. A fiberoptic endoscope has an eyepiece, while a video endoscope has remote control buttons for the video control unit (Fig. 1.5).
Supply plug and umbilical cord. The supply plug at the end of the umbilical cord has distal connectors for the light guide and air supply, side connectors for the water bottle and suction, and an air vent, which is not functional during endoscopy. The umbilical cord connects the supply plug to the control head.
Control head and insertion tube. Between the umbilical cord and insertion tube is the control head, which has controls for air insufflation, irrigation, suction, and for the bending section at the distal end of the scope. At the intersection of the insertion tube and control head, there is a biopsy port for passing instruments down the endoscope shaft. The insertion tube has a distal bending section, whose tip carries the illuminating end of the light guide, air and water jets, the distal opening of the biopsy channel, and the lens or video chip.
Endoscope handling and operation are described elsewhere (see p. 18).
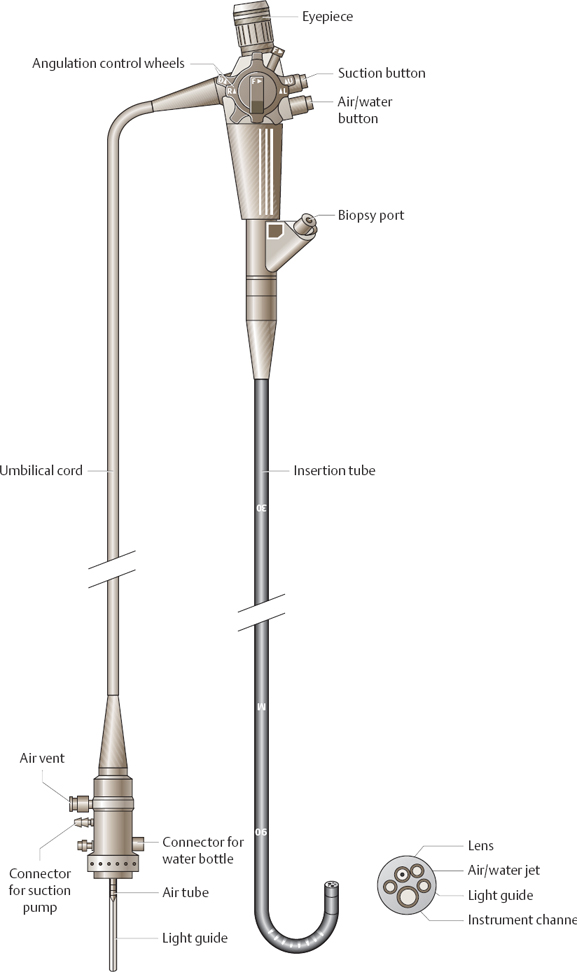
Fig. 1.5 Endoscope
Fiberoptic vs. Video Endoscopy
In a fiberoptic endoscope, light is conducted from the distal lens to the eyepiece by bundles of optical glass fibers. In a video endoscope, the image is captured with a video chip at the distal end of the endoscope, transmitted electronically, and displayed on a monitor.
Advantages and disadvantages. Video endoscopy offers several advantages: high resolution; the convenience of a monitor display, which permits others in the room to view the image; easier handling of the endoscope during the procedure; and easier documentation of images, which can be digitally processed and stored. The main disadvantage of video endoscopy is its high cost.
A video camera can also be coupled to the eyepiece of a conventional fiberoptic endoscope, providing a monitor display. But the image quality is markedly reduced compared with direct video endoscopy.
Endoscopy Suite: Accessories
 Endoscopic Accessories
Endoscopic Accessories
The great advantage of endoscopy lies in the option of using both diagnostic and therapeutic instruments in one session. The necessary endoscopic accessories will depend on the requirements of the endoscopy department. Standard accessories consist of irrigation and suction tubes, cytology brushes, biopsy forceps, foreign-body retrieval forceps, and injection needles. Optional accessories include polypectomy snares, extraction baskets, dilators, and dilation sets.
 Emergency Equipment
Emergency Equipment
Upper GI endoscopy should be performed only if proper emergency supplies are within reach. The items listed in Table 1.5 should be available.
Necessary emergency medications are listed in Table 1.6.
 Documentation of Findings
Documentation of Findings
The cornerstone of documentation is the written endoscopy report. Images documenting abnormal findings and even normal findings in selected cases are a desirable adjunct to the written report.
Image documentation. Selected images can be printed out on a video printer. Documentation on videotape can provide a complete record of the examination procedure and findings, but videotapes can be costly to archive. A standard written report that gives a brief description of all inspected areas, including normal findings, is unsurpassed for its reproducibility and its value as a baseline for future examinations.
Guidelines for endoscopic reporting are provided on page 182 ff.
|
 Suction apparatus
Suction apparatus Oxygen
Oxygen Intubation set
Intubation set Ventilation bag
Ventilation bag Defibrillator
Defibrillator Pulse oximeter
Pulse oximeter ECG monitor
ECG monitor Sphygmomanometer
Sphygmomanometer Indwelling venous cannula
Indwelling venous cannula Sengstaken tube
Sengstaken tube Sclerosant
Sclerosant | Atropine | Atropine, 0.5-mg ampules |
| Epinephrine | Suprarenin, 1-mL ampules 1:1000 |
| Flumazenil | Anexate, 0.5-mg ampules |
| Lidocaine | Xylocaine, 0.5%5mL |
| Naloxone | Narcanti, 0.4-mg ampules |
| Theophylline | Euphyllin, 240-mg ampules |
| Prednisolone | Solu-Decortin, 250-mg ampules |
| Nitro spray | Nitrolingual Spray |
| Nifedipine | Adalat capsules |
| Clemastine | Tavegil, 2-mg ampules |
| Infusion solutions |
Preparations for Endoscopy: Informed Consent
 Disclosure and Informed Consent
Disclosure and Informed Consent
Disclosure should be taken very seriously. It is generally known that the great majority of lawsuits brought by patients against physicians stem from inadequate disclosure rather than treatment errors. Despite its relatively high tolerance and low complication risks, upper GI endoscopy is still an invasive examination. The patient should sign a consent form confirming that the physician has fully explained the nature and risks of the procedure, and the consent form should accurately reflect the information that the patient has received.
General Policies
 Disclosure is provided by a physician.
Disclosure is provided by a physician.
 Disclosure should be given at least 24 hours prior to the examination.
Disclosure should be given at least 24 hours prior to the examination.
 Disclosure is given verbally and in writing (aided by a standard information sheet).
Disclosure is given verbally and in writing (aided by a standard information sheet).
 The consent form should reflect the information that has been disclosed.
The consent form should reflect the information that has been disclosed.
 The patient willingly consents to the procedure in writing.
The patient willingly consents to the procedure in writing.
Exceptions
 Disclosure may be waived for patients who are not verbally responsive.
Disclosure may be waived for patients who are not verbally responsive.
 Disclosure may be waived in emergencies and for incompetent patients.
Disclosure may be waived in emergencies and for incompetent patients.
Content of Disclosure
Adequate disclosure should include the reasons for performing the examination and the details of the procedure itself, patient-associated risks and special circumstances, the risks of the examination and of medications used during the procedure, and patient instructions before and after the examination.
General information about the procedure
 Reason for the examination
Reason for the examination
 Nature and conduct of the examination
Nature and conduct of the examination
 Alternatives
Alternatives
 Possible consequences of refusing the procedure
Possible consequences of refusing the procedure
 Risks and discomfort
Risks and discomfort
Patient
 Patient risk factors
Patient risk factors
 Allergies
Allergies
 Prior illnesses
Prior illnesses
 Bleeding tendency
Bleeding tendency
 Dental status
Dental status
 Prior surgery
Prior surgery
 Medications that are taken regularly
Medications that are taken regularly
Patient instructions before and after the procedure
 Nothing by mouth for 12 hours before the examination.
Nothing by mouth for 12 hours before the examination.
 No solid foods for 30 minutes after the examination.
No solid foods for 30 minutes after the examination.
 Allow for aftereffects of sedation (no driving, no hazardous work activities for 24 hours).
Allow for aftereffects of sedation (no driving, no hazardous work activities for 24 hours).
 Report any complications (pain, bleeding, fever).
Report any complications (pain, bleeding, fever).
Risks and complications
 Complication rate of diagnostic endoscopy
Complication rate of diagnostic endoscopy
– Overall complication rate < 0.1 %
– Mortality < 0.01 %
 Cardiac complications
Cardiac complications
– Ischemia, arrhythmias
 Pulmonary complications
Pulmonary complications
– Hypoxia, aspiration
 Bleeding and perforation
Bleeding and perforation
 Infection
Infection
 Complications from medications used during the procedure
Complications from medications used during the procedure
– Pharyngeal anesthesia: allergy, aspiration
– Sedation: respiratory depression, hypotension
 Complications of therapeutic endoscopy (sclerotherapy of esophageal varices, bougie or balloon dilation of the esophagus, polypectomy)
Complications of therapeutic endoscopy (sclerotherapy of esophageal varices, bougie or balloon dilation of the esophagus, polypectomy)
– Bleeding, perforation, mediastinitis, fistulation, pleural effusion
 Complications of percutaneous endoscopic gastrostomy (PEG) placement and percutaneous endoscopic jejunostomy (PEJ) placement
Complications of percutaneous endoscopic gastrostomy (PEG) placement and percutaneous endoscopic jejunostomy (PEJ) placement
– Local infection, peritonitis, bleeding, sepsis
Preparations for Endoscopy: Medications (1)
 Premedication and Medications Used During the Procedure
Premedication and Medications Used During the Procedure
It is not strictly necessary to premedicate or medicate patients for upper GI endoscopy. The use and selection of medications should be tailored to the individual case. The following types of medication may be used:
 Local anesthetics
Local anesthetics
 Sedatives
Sedatives
 Analgesics Narcotics
Analgesics Narcotics
 Antispasmodics
Antispasmodics
 Defoaming agents
Defoaming agents
Local Anesthesia
Indication
 Pharyngeal anesthesia can be used in any endoscopic procedure.
Pharyngeal anesthesia can be used in any endoscopic procedure.
Contraindications
 Emergency endoscopy (increased risk of aspiration)
Emergency endoscopy (increased risk of aspiration)
 Known hypersensitivity
Known hypersensitivity
Advantage
 Better patient tolerance of the examination
Better patient tolerance of the examination
Disadvantages
 Increased risk of aspiration
Increased risk of aspiration
 Allergic reaction
Allergic reaction
 Bad taste
Bad taste
 Cough
Cough
 Swallowing difficulties after the examination
Swallowing difficulties after the examination
Method
 Two squirts of lidocaine sprayed into the pharynx
Two squirts of lidocaine sprayed into the pharynx
Precautions
 Nothing by mouth from 30 minutes to one hour after the examination
Nothing by mouth from 30 minutes to one hour after the examination
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


