Over the past 20 years, there has been a gradual evolution in the treatments offered to patients with head and neck squamous cell cancer (HNSCC). Although 60 to 80% of patients with early-stage I and II HNSCC can be cured with surgery and/or radiation therapy, the cure rate falls to 30% or less for patients with locally advanced stage III and IV disease. Local and regional relapse accounts for most of the failures observed in patients treated with surgery and radiation therapy. A few patients experience distant tumor spread. Chemotherapy, historically used for palliation in patients with recurrent and/or metastatic disease, has been investigated in several experimental multimodality primary treatment regimens. These investigations have attempted to improve survival, locoregional control, and organ preservation. Distant failure rates and quality of life have also been evaluated. Although surgery and radiotherapy are the most accepted primary treatments for patients with locally advanced HNSCC, recent literature, including meta-analyses of randomized studies, suggests that concomitant chemo- and radiotherapy, with or without surgery, has become the new standard. This chapter briefly reviews the traditional role of chemotherapy for the palliation of recurrent and/or metastatic disease and then describes the recent studies that show a role for chemotherapy in the front-line treatment of patients with locally advanced disease. Background TREATMENT OF RECURRENT OR METASTATIC DISEASE The use of chemotherapy to treat patients with incurable metastatic or recurrent HNSCC is well established. The median survival for these patients is approximately 6 months, and chemotherapy has had little impact on overall survival. The goal of this treatment is palliation of cancer-related symptoms attributable to a reduction in tumor burden. Multiple chemotherapeutic regimens using single agents and combinations of effective drugs have been investigated. Tumor response, time to progression, and overall survival time are the endpoints most frequently reported. Tumor responses include complete responses (CR, i.e., the disappearance of all measurable disease) and partial responses (PR, i.e., 50% reduction in measurable disease). Quality of life is becoming an additional valued endpoint. Single-Agent Chemotherapy Multiple single agents have efficacy in the treatment of HNSCC (Table 7-1). Methotrexate is frequently listed as the standard treatment for metastatic and recurrent HNSCC. The drug is given weekly by intravenous infusion, with mucositis and myelosuppression the dose-limiting toxicities. Although initial response rates of 30% were reported, a large multi-institutional randomized study reported a response rate of only 10%.
| Chemotherapy | Pooled Response Rate (%) a |
| Methotrexate | 31 |
| Cisplatin | 28 |
| Carboplatin | 22 |
| Bleomycin | 21 |
| Paclitaxel | 40 |
| Docetaxel | 31 |
| 5-Fluorouracil | 15 |
| Ifosfamide | 26 |
| Topotecan | 22 |
| Vinorelbine | 22 |
| Gemcitabine | 13 |
a Includes both complete remission (CR) and partial remission (PR).
Cisplatin is one of the most active agents used in the treatment of HNSCC. Response rates of 14 to 41% and a pooled average response rate of 28% have been reported. Nephrotoxi-city, neurotoxicity, and ototoxicity, coupled with significant nausea and vomiting, are the major toxicities associated with cisplatin. The cisplatin analogue, carboplatin, may have less toxicity. Response rates for carboplatin are 14 to 30%, with a pooled average of 22%.
The taxanes, paclitaxel (Taxol) and docetaxel (Taxotere), have shown impressive response rates of 30 to 40% in patients with recurrent HNSCC. The major toxicities of these agents include myelosuppression, peripheral neuropathy, mucositis, and hypersensitivity.
5-FU has been studied extensively in a variety of doses and schedules. Mucositis is the primary dose-limiting toxicity. Although it has a significant role in combination chemotherapy for HNSCC, the pooled single-agent response rate by continuous infusion is only 15%.
Other single agents that have activity in HNSCC are ifosfamide, vinorelbine, and gemcitabine.
Combination Chemotherapy
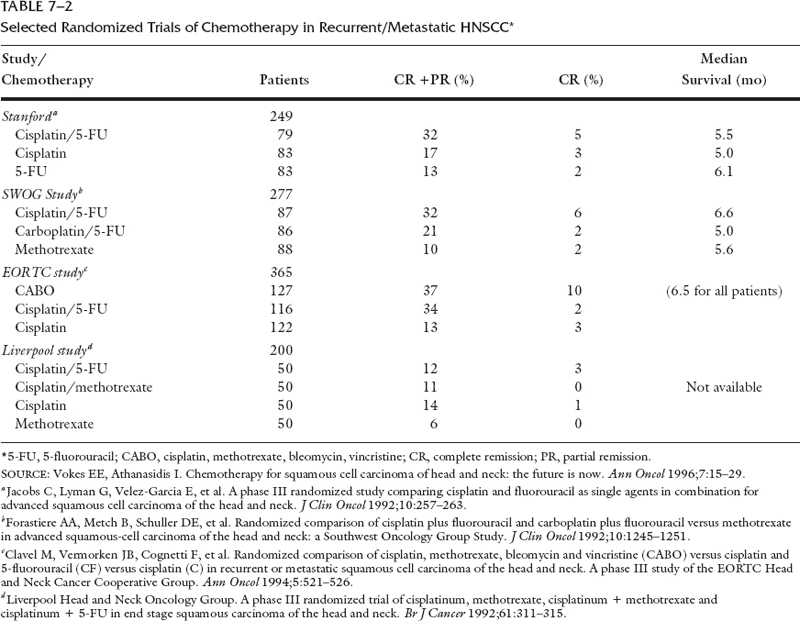
Combination chemotherapy for metastatic and recurrent HNSCC has been studied extensively. The combination of cisplatin and 4 to 5 days of continuous infusion of 5-FU (PF) has been shown in single-institution trials to produce response rates as high as 70%. Four large randomized studies1, 2, 3, 4 (Table 7-2) have compared this regimen with single-agent and alternative combination therapies. The response rates from these studies were approximately 30%. Although early studies suggested that the addition of interferon-α2b (IFN-α2b) to PF might lead to improved response, a randomized study demonstrated increased toxicity without improvement in response or survival.
A 1994 study of standard chemotherapy for metastatic and recurrent HNSCC analyzed 15 randomized studies of single-agent and combination therapy.5 The authors concluded that although the combination of cisplatin and 5-FU produced a higher response rate and a possible limited improvement in survival, this came at the expense of significant additional toxicity.
Recently, single-institution taxane-based combination therapy has yielded encouraging responses rates. A phase II study of paclitaxel, ifosfamide, and cisplatin (TIP)6 in patients with recurrent or metastatic disease reported an overall response rate of 58% with a 17% complete response rate, and a median survival of 8.8 months. These newer drug combinations will have to be compared in multi-institution randomized studies before any firm conclusions can be reached.
TREATMENT OF INITIAL LOCOREGIONALLY ADVANCED DISEASE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


