Fundus Autofluorescence in Best Disease
Markus Preising
Best disease was first reported in 1905 as a disease affecting the macula (1). The initial report was on eight members of one family from Giessen with mixed bilateral and unilateral disease presenting with a clearly demarcated macular lesion below the fovea of light red to yellow-white color, which Best described as completed central “choroiditis.” Various stages of the lesion were recognized as showing rectangular and crescent-shaped forms (1). These stages were later classified by Gass et al. (2). Currently, five stages are generally accepted (Fig. 11F.1):
Previtelliform stage: No fundus abnormalities; mutation carriers are in this stage and will not be recognized if the family does not present with a history of Best disease (Fig. 11F.1A,B).
Vitelliform stage: Prominent, yellow or light red, well-demarcated central macular lesion that, over time, increases in size to occupy the entire macular area; the lesion is circular and the color is quite uniform (Fig. 11F.1C,D). This stage was the primary stage described by Best (1).
Pseudohypopyon stage: The yellowish material occupies predominantly the lower half of the lesion (Fig. 11F.1E,F).
Vitelliruptive or “scrambled egg” stage: The lesion develops an elliptical shape in the vertical axis that is described in association with a loss of visual acuity and disruption of the uniform distribution of the yellowish material, which appears, at this stage, to precipitate in the subretinal space and at the margins of the lesion (Fig. 11F.1G,H).
Fibrotic stage: Corresponds to the complete “choroiditis” described by Best (1) in which there is cicatrization of the macula and subretinal fibrosis. A minimal amount of yellow material may still be visible within the scar (Fig. 11F.1I,J).
The age of onset of the disease, the progression through the different stages, and the penetrance of the symptoms is very variable among different families. Symptoms may appear in the first decade of life or may never develop, as it occurs in carriers of the disease. The disease may initially affect one eye only, with both eyes later progressing independently. Some patients may have lesions in the vitelliform stage that remain unchanged for many years, whereas others may progress to the pseudohypopyon stage within a few months. This heterogeneity in the progression of the disease was originally recognized by Best (1) and confirmed in several later reports, including our own studies (3).
MOLECULAR BASIS AND HISTOPATHOLOGY
Human Best1 gene (hBEST1) codes for a protein (bestrophin) involved in transmembrane transport in membranes of the retinal pigment epithelium (RPE). The gene product
is part of a Ca2+-activated Cl− channel (CACC). Bestrophin was considered to be the channel itself (4), but its functional characteristics did not support the notion that bestrophin acts as a Cl− channel (5). Recent studies have solved the problem by showing that bestrophin interacts with β-subunits of the channel, influencing the activity of the CACC, and thus explaining the functional characteristics of bestrophin (6). Histological studies locate bestrophin on the basolateral side of the RPE, and the common notion was that the protein is part of the basolateral membrane (7). Expression is
higher in the extramacular than in the macular RPE, as shown based on protein and RNA levels (8). The question of the functional impact and pathological effect remains to be resolved. As a first hypothesis. Fischmeister and Hartzell (9) proposed that bestrophin is involved in a cell volume-dependent current that decreases when the volume of the RPE cell increases. Such an increase in volume may be caused by osmotic stress in the interphotoreceptor space, or follow phagocytotic activity when the RPE clears the shaded outer segments at night. In this regard, phagocytosis may be hampered by the imbalanced osmotic equilibration caused by improper bestrophin function (9).
is part of a Ca2+-activated Cl− channel (CACC). Bestrophin was considered to be the channel itself (4), but its functional characteristics did not support the notion that bestrophin acts as a Cl− channel (5). Recent studies have solved the problem by showing that bestrophin interacts with β-subunits of the channel, influencing the activity of the CACC, and thus explaining the functional characteristics of bestrophin (6). Histological studies locate bestrophin on the basolateral side of the RPE, and the common notion was that the protein is part of the basolateral membrane (7). Expression is
higher in the extramacular than in the macular RPE, as shown based on protein and RNA levels (8). The question of the functional impact and pathological effect remains to be resolved. As a first hypothesis. Fischmeister and Hartzell (9) proposed that bestrophin is involved in a cell volume-dependent current that decreases when the volume of the RPE cell increases. Such an increase in volume may be caused by osmotic stress in the interphotoreceptor space, or follow phagocytotic activity when the RPE clears the shaded outer segments at night. In this regard, phagocytosis may be hampered by the imbalanced osmotic equilibration caused by improper bestrophin function (9).
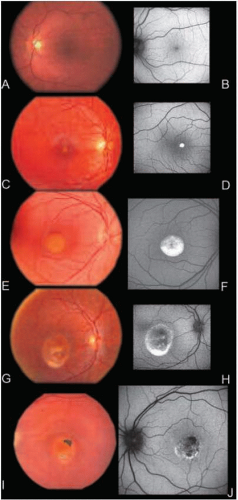 FIGURE 11F.1. Fundus photographs (A,C,E,G,I) and fundus AF images (B,D,F,H,J) of five patients with various stages of Best disease. A clinical heterogeneity with regard to the age of onset and the progression of the disease is manifested in these photographs of a 39-year-old patient in the previtelliform stage (A,B), a 6-year-old patient in the vitelliform stage (C,D), an 8-year-old patient in the early pseudohypopion stage (E,F), a 16-year-old patient in the vitelliruptive stage (G,H), and a 17-year-old patient in the fibrotic and final stage of the disease (I,J). |
Best disease (VMD2) segregates in an autosomal dominant way. Reduced penetrance has been associated with certain mutations, including c.969delTCA, a very frequent in-frame deletion (3).
Patients affected by Best disease present to the ophthalmologist with decreased visual acuity and color vision deficits, or ask for an appointment for genetic counseling due to a positive family history. In carriers and in patients up to the vitelliform stage of the disease, the reduction of visual acuity may not be as prominent as the fundus changes would suggest. A rapid drop in visual acuity occurs when the patient progresses through the vitelliruptive stage, although useful visual acuity may be retained into the fibrotic stage (3). Visual acuity depends on surviving photoreceptor cells and a preserved photoreceptor cell layer on which the image can be mapped. Any change in surface, receptor density, and receptor distribution will lead to faulty image mapping. A faulty image mapping reduces visual acuity. The faulty mapping may be tolerated to a certain extent by the adaptability of the visual system and may be recognized by the patient in later stages of the disease only. Especially when photoreceptor loss becomes profound in the fibrotic stage or rearrangements of the photoreceptor layer take place in vitelliruptive stage, the visual acuity will drop (3,10).
The lesion described by Best was seen on fundus photographs to be located under the fovea and within the retinal layers (1). Histological studies dating from the 1980s reported on cases in the vitelliruptive (11) and fibrotic (12) stages. These studies localized the lesion to the level of the RPE. Weingeist et al. (12) described accumulation of vesicles in the RPE below the lesion that stained with lipophilic substances on light microscopy. These vesicles were distributed throughout the cells and identified as lipofuscin granules (11,13).
The histology of an eye from a patient in a late stage of the disease and with a known hBEST1 mutation (T6R) supported the results of Weingeist et al. (12). The results showed that accumulation of lipofuscin granules occurred peripheral to the scar region and that, beneath the scar, the RPE was atrophic with only rare inclusions (8). Results from a 93-year-old patient with peripheral flecks carrying a Y227N mutation contradicted the findings in the T6R patient concerning lipofuscin accumulation. The Y227N mutation was associated with normal distribution of AF in the macular region. Mullins et al. (8) judged this as a variability of phenotypical expression. Lipofuscin density was studied in purified intracellular granules in a further patient carrying a homozygous missense mutation (W93C) in hBEST1 compared with a heterozygous individual carrying the T6R mutation (8) and age-matched controls (13). The severity of the disease was no higher in the patient carrying the homozygous mutation. Both patients showed a reduction of the classical lipofuscin fraction of light dense granules. A shift to denser lipofuscin granules was noted by fluorescence measurements of fractionated RPE granules (13). The denser granules were multilobed, indicating fusion of lipofuscin granules and thus impaired trafficking of lipofuscin granules within the RPE as a result of the dysfunction of bestrophin.
Some additional features were noted, such as a reduced number of melanosomes and an increased amount of secondary lysosomes. Mitochondria showed abnormal torpedo-like shapes and small electron dense particles were shown in the extracellular
space enmeshed in a fine fibrillar substance (12). Hypertrophy of the ER was reported in a further case, as well as loss of fenestration and occurrence of ghost vessels in the choriocapillaris (8).
space enmeshed in a fine fibrillar substance (12). Hypertrophy of the ER was reported in a further case, as well as loss of fenestration and occurrence of ghost vessels in the choriocapillaris (8).
IMAGING AND DIAGNOSTIC TECHNIQUES
Best disease is a macular disorder with prominent and characteristic features seen on fundus photography (see Introduction). The diagnosis of Best disease is usually made by slit-lamp biomicroscopy, taking into account visual acuity, color vision, and visual field findings. Functional testing, especially electro-oculography (EOG), is often obtained to confirm the diagnosis.
Fluorescein and Indocyanine Green Angiography
Angiography is only rarely used to evaluate patients with Best disease. Since fluorescein angiography (FA) displays the retinal vasculature, its application may be useful to discern elder and late-stage Best disease patients from patients with adult vitelliform macular dystrophy (AVMD) and age-related macular degeneration (AMD). The latter show leakage of retinal vessels throughout the retina by FA, whereas in patients with Best, the fluorescein leakage is restricted to the macular lesion. Few reports on the use of indocyanine green (ICG) angiography in patients with Best disease are available (14,15). Maruko et al. (14) found many hyperfluorescent spots in the peripheral and midperipheral retina on ICG angiography in patients with confirmed mutations in hBEST1. The hyperfluorescent spots in the periphery did not correspond to vitelliform lesions resulting from lipofuscin accumulation. This was shown by AF of the peripheral vitelliform lesions. Maruko et al. (14) concluded that the diffuse hyperfluorescent spots seen on ICG angiography were located on the RPE/Bruch’s membrane level and were associated with fibrillar and drusenoid material. Quaranta et al. (15) focused their fluorescein and ICG angiography on the macular lesion, showing the diffuse hyperfluorescent spots also reported by Maruko et al. (14). Quaranta et al. (15) did not report on any mutation in hBEST1 in the patients presented. Both groups showed that fluorescence in the macula did not occur on FA but resulted from the AF inside the lesion (15). Finally, Pollack et al. (16) reported the FA findings in a case of Best disease with positive mutation detection. In that report, hyperfluorescent spots were presented at the macula corresponding to light spots of yellowish material in the macular lesion. FA is helpful in detecting the rare occurrence of choroidal neovascularization (CNV) in patients with Best disease, especially in those in advanced stages of the disease.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


