Purpose
To review and interpret the anatomy of the optic nerve head (ONH) detected with spectral-domain optical coherence tomography (SD OCT) pertaining to the clinical examination of the optic disc and to propose that a paradigm change for clinical assessment of the ONH is necessary.
Design
Perspective.
Methods
Presently, the clinician evaluates neuroretinal rim health according to the appearance of the optic disc, the clinically visible surface of the ONH. Recent anatomic findings with SD OCT have challenged the basis and accuracy of current rim evaluation. We demonstrate why incorporation of SD OCT imaging of the ONH into the clinical examination of the disc is required.
Results
Disc margin-based rim evaluation lacks a solid anatomic basis and results in variably inaccurate measurements for 2 reasons. First, the clinically visible disc margin is an unreliable outer border of rim tissue because of clinically and photographically invisible extensions of Bruch’s membrane. Second, rim tissue orientation is not considered in width measurements. We propose alternative anatomically and geometrically accurate SD OCT-based approaches for rim assessment that have enhanced detection of glaucoma. We also argue for new data acquisition and analysis strategies with SD OCT that account for the large interindividual variability in the angle between the fovea and ONH.
Conclusions
We propose a 4-point paradigm change for clinical assessment of the ONH that is anchored to the eye-specific anatomy and geometry of the ONH and fovea. Our approach is designed to enhance the accuracy and consistency of rim width, as well as of peripapillary and macular intraretinal thickness measurements.
Since von Helmholtz’s description of the direct ophthalmoscope in 1851, clinical examination of the optic disc has been a cornerstone of ophthalmic practice. The optic disc constitutes the clinically visible surface of the neural and connective tissues of the optic nerve head (ONH). By current convention, clinical disc examination requires identification of the outer and inner borders of the neuroretinal rim, respectively, the optic disc margin, and the optic disc cup. The amount of rim tissue then is estimated within the apparent plane of the disc margin as either the ratio of the size of the cup to the size of the disc or the rim area. These concepts are applied whether the examination is performed with direct ophthalmoscopy, slit-lamp biomicroscopy, optic disc photography, or a growing number of quantitative imaging methods.
Advances in spectral-domain optical coherence tomography (SD OCT) for the first time have permitted imaging of ONH anatomic features. Structures such as the anterior and posterior lamina cribrosa surfaces, Bruch’s membrane–retinal pigment epithelium complex and its termination within the ONH, border tissue of Elschnig, and the scleral canal opening now can be visualized readily. Accurately colocalizing fundus photographs to SD OCT image data has allowed clinicians to identify structures that correspond to common clinical landmarks, for example, the optic disc margin.
In this article, we explain how recent SD OCT findings undermine the current concepts of the clinical disc margin and rim quantification from both anatomic and geometric perspectives. In light of these findings, we propose a 4-part paradigm for incorporating new insights provided by SD OCT imaging of ONH anatomic features into the clinical examination of the optic disc to achieve a clinical assessment of the ONH. The paradigm recognizes the variable relationship between the fovea, the path of the retinal nerve fiber bundles, and the ONH among individuals. Its logic links the evaluation of the neuroretinal rim and peripapillary and macular retinal nerve fiber layer (RNFL) to the specific anatomy and geometry of each individual ONH and its relative orientation with the fovea.
Anatomic Assumptions Underlying the Clinically Visible Optic Disc Margin
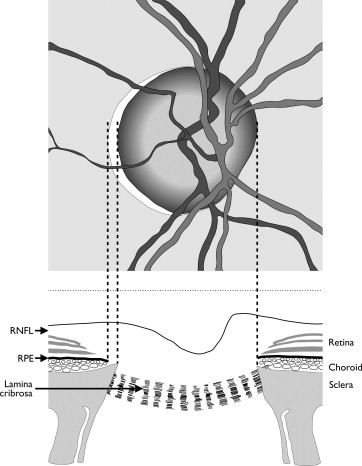
The optic disc margin is a clinical landmark that traditionally is defined to be the inner edge of the scleral lip or crescent ( Figure 1 ). Within this conceptual framework, the disc margin is assumed to be a single and consistent anatomic structure around the entire ONH and a true outer border of the neuroretinal rim, and therefore the landmark from which the width of the rim can be measured. Current examination methods require identification of the disc margin, whether the examination is performed clinically, photographically, or with confocal scanning laser tomography, an imaging technique that maps the surface topography of the ONH.
Anatomic Errors in the Current Evaluation of the Neuroretinal Rim
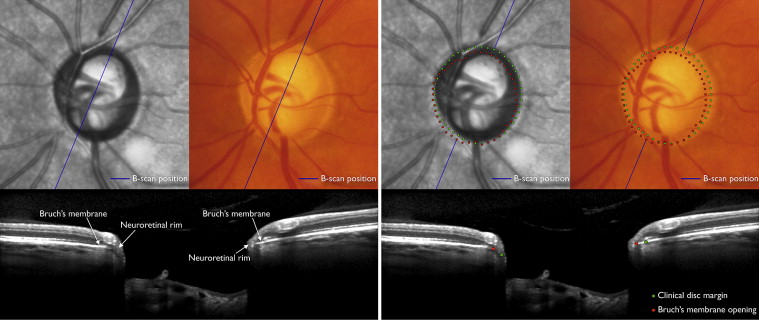
Recent histologic findings in monkey eyes and SD OCT findings in human eyes (in each case, colocalized to optic disc stereophotographs with the disc margin traced by a glaucomatologist) have revealed 2 new findings that challenge the anatomic assumptions that underlie optic disc margin-based neuroretinal rim evaluation. First, the clinical disc margin rarely is a single anatomic entity, nor are the structures that underlie it consistent in an individual eye. Hence, the structure corresponding to the disc margin at the 3-o’clock position may be different to that at the 9-o’clock position. Similarly, the structure corresponding to it at the 3-o’clock position in 2 eyes also may be different. Second, what the clinician perceives as the disc margin in clinical examination or with photographs frequently is not a true anatomic outer border of the neuroretinal rim because of regionally variable and invisible extensions of Bruch’s membrane that have not been appreciated previously ( Figure 2 ). In such cases, there can be a serious overestimation of the remaining rim tissue.
Separate from these new issues regarding the anatomic outer border of the neuroretinal rim, its inner border, which constitutes the cup margin, is evaluated clinically with a stereoscopic evaluation of the rim width within the perceived plane of the disc margin. However, the rationale to support the existence of an anatomically defensible junction between the neuroretinal rim and cup is weak. Current imaging techniques similarly divide the rim and cup on the basis of an arbitrary depth below a fixed plane.
The consequence of these findings is that current parameters, including cup-to-disc ratio and neuroretinal rim area, are unlikely to estimate accurately the amount of remaining neural tissue in the ONH.
Anatomic Errors in the Current Evaluation of the Neuroretinal Rim
Recent histologic findings in monkey eyes and SD OCT findings in human eyes (in each case, colocalized to optic disc stereophotographs with the disc margin traced by a glaucomatologist) have revealed 2 new findings that challenge the anatomic assumptions that underlie optic disc margin-based neuroretinal rim evaluation. First, the clinical disc margin rarely is a single anatomic entity, nor are the structures that underlie it consistent in an individual eye. Hence, the structure corresponding to the disc margin at the 3-o’clock position may be different to that at the 9-o’clock position. Similarly, the structure corresponding to it at the 3-o’clock position in 2 eyes also may be different. Second, what the clinician perceives as the disc margin in clinical examination or with photographs frequently is not a true anatomic outer border of the neuroretinal rim because of regionally variable and invisible extensions of Bruch’s membrane that have not been appreciated previously ( Figure 2 ). In such cases, there can be a serious overestimation of the remaining rim tissue.
Separate from these new issues regarding the anatomic outer border of the neuroretinal rim, its inner border, which constitutes the cup margin, is evaluated clinically with a stereoscopic evaluation of the rim width within the perceived plane of the disc margin. However, the rationale to support the existence of an anatomically defensible junction between the neuroretinal rim and cup is weak. Current imaging techniques similarly divide the rim and cup on the basis of an arbitrary depth below a fixed plane.
The consequence of these findings is that current parameters, including cup-to-disc ratio and neuroretinal rim area, are unlikely to estimate accurately the amount of remaining neural tissue in the ONH.
Anatomic Rationale for Bruch’s Membrane Opening as the Outer Border of the Neuroretinal Rim
The termination of bruch’s membrane at the ONH represents the opening through which retinal ganglion cell axons exit the eye to form the choroidal and scleral portions of the neural canal. As such, this anatomic opening, termed Bruch’s membrane opening (BMO), is a true outer border of the neural tissues because axons cannot pass through an intact Bruch’s membrane to exit the eye. Whether BMO is clinically visible, it is an anatomically accurate landmark from which neuroretinal rim measurements can be made. It is also a structure that is identified consistently with SD OCT.
The stability of BMO under a variety of conditions provides another rationale for its usefulness as a landmark. BMO is unaltered in the face of large changes in intraocular pressure induced by glaucoma surgery. The 2-dimensional plane that best fits BMO also is axially stable with surgical reduction of intraocular pressure. There is no published evidence yet on the stability of BMO with glaucoma progression; however, in experimental glaucoma in monkeys, BMO position in 3-dimensional histomorphometry of the ONH seems to be unaltered despite changes in the neural component of the ONH and in the positions of the anterior and posterior scleral canal opening.
Geometric Errors in the Current Evaluation of the Neuroretinal Rim
Neuroretinal rim measurement with clinical, photographic, or confocal scanning laser tomographic techniques is made along the 2-dimensional plane of the perceived optic disc margin. However, in a single eye, the orientation of rim tissue varies around the ONH. At one extreme, axons may exit the eye almost parallel to the visual axis, whereas at the other extreme, they may exit the eye almost perpendicular to it, typically in the temporal sector, which can have a shallow sloping rim. Hence, potentially significant errors in rim width can occur if the measurement plane is fixed. For example, for the same number of axons, the conventional rim width will be larger when its orientation is more horizontal compared with when it is more perpendicular to the fixed plane of measurement ( Figure 3 ). Even if a rim measurement is made from an anatomically accurate location, that is, BMO, its width along the approximately horizontal fixed plane of BMO will be influenced by the orientation of the overlying rim tissue ( Figure 3 ).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


