Purpose
Cavitary optic disc maculopathy develops when fluctuating pressure gradients along anomalous communications in the optic nerve head induce migration of fluid into the adjacent retinal tissue. We sought to determine whether carefully titrated laser photocoagulation combined with vitrectomy and gas tamponade can safely create an effective intraretinal barrier to fluid egress from the optic disc cavitation.
Design
Retrospective interventional case series.
Methods
We retrospectively evaluated medical records and imaging studies of 22 consecutive patients with cavitary disc maculopathy evaluated by a single surgeon between 1991 and 2014. Patients requiring surgery underwent carefully titrated juxtapapillary laser photocoagulation followed immediately by vitrectomy and gas tamponade. Main outcome measures were change in visual acuity, macular fluid resolution, and recurrence of maculopathy.
Results
Eleven patients (11 eyes) had undergone vitreous surgery and were included in the study. No preoperative evidence for vitreous traction on the optic disc or macula was seen in any eye. Nine patients underwent a single surgery and 2 patients required additional procedures to resolve the macular fluid. Mean length of follow-up after the last surgery was 48.2 months (range, 4–143 months). All 11 patients (100%) had complete resolution of macular fluid, with an average time to resolution of 8.5 months (range, 1–18 months). Only 1 of 11 patients (9%) had recurrence of macular fluid (14 months postoperatively). The average preoperative visual acuity of 20/125 (logMAR 0.81, standard deviation [SD] = 0.36) improved by nearly 4 lines to an average final visual acuity of 20/57 (logMAR 0.45, SD = 0.37) ( P = .0072). A possible laser-induced central scotoma was suspected in only 1 patient who had undergone extensive prior laser treatments.
Conclusions
An effective intraretinal barrier to fluid migration from cavitary optic disc anomalies can be safely achieved in most patients with carefully titrated juxtapapillary laser photocoagulation combined with vitrectomy and gas tamponade. Once achieved, the barrier facilitates resolution of macular fluid and long-term avoidance of recurrent maculopathy.
The association of serous maculopathy with cavitary optic disc anomalies has long been known, but attempts at surgical repair are often frustrated by persistent or recurrent maculopathy, in part owing to a lack of understanding of the underlying pathogenesis. Typical and atypical optic disc coloboma, optic pit, morning glory disc anomaly, and extrapapillary cavitation comprise a continuum of anomalies that may arise from failure of the optic fissure to close during embryogenesis. In such eyes, dysplastic retina herniates through a defect in the sclera and/or lamina cribrosa. Over 50% of eyes with cavitary disc anomalies develop localized serous maculopathy. Clinical examination and optical coherence tomography (OCT) of these eyes reveal that there is an accumulation of intraretinal and/or subretinal fluid contiguous with the cavitary anomaly that may progress to obvious serous detachment of the macula. In eyes with cavitary disc maculopathy, the natural history is one of visual decline, with 1 study reporting that the majority of untreated patients progress to visual acuities of 20/200 or worse.
The pathophysiologic mechanisms responsible for cavitary disc maculopathy remain unclear. Several authors have suggested a possible pathogenic role for vitreous traction. However, as recently discussed, there are serious limitations to the vitreous traction hypothesis and it fails to account for many of the unusual features of this disorder. Rather, we believe that cavitary disc maculopathy develops when fluctuating pressure gradients along anomalous communications in the optic nerve head induce migration of liquid vitreous and/or cerebrospinal fluid into the adjacent retinal tissue. Although the fluid can enter the retina at various levels, it most commonly migrates into the outer nuclear layer and only rarely enters directly into the subretinal space. In theory, then, an effective blockade of fluid passage from the cavitary anomaly into the macula must consist primarily of an intraretinal , not just a subretinal, barrier to fluid migration. We hypothesized that carefully titrated laser photocoagulation combined with vitrectomy and gas tamponade can safely create an effective intraretinal barrier to fluid egress from the optic disc cavitation and thereby provide a long-term cure of the associated maculopathy.
Methods
This study was a retrospective interventional case series performed at a single academic institution. The Institutional Review Board at the University of Michigan approved a retrospective evaluation of medical records and imaging studies of consecutive patients with cavitary disc maculopathy. We identified 22 such patients evaluated by a single surgeon between 1991 and 2014. Those patients that had undergone vitreoretinal surgery for this condition at our center were included in this study. Each patient gave full informed consent prior to surgery, and the research study complied with Health Insurance Portability and Accountability Act guidelines.
The first step in the treatment procedure consisted of carefully titrated juxtapapillary laser photocoagulation, which was typically performed at the slit lamp immediately prior to the vitrectomy procedure. Using a high-magnification fundus contact lens, red wavelength laser was applied to the temporal juxtapapillary fundus, starting approximately 1 burn width away from the edge of the optic nerve. Typical laser parameters were 0.2 seconds and 200 μm spot size, using a red (647 nm) laser wavelength. The energy was carefully titrated so as to produce a moderate gray-white burn at the level of the outer retina and retinal pigment epithelium (RPE) with thermal spread into the middle layers of the retina, but carefully avoiding the nerve fiber layer ( Figure 1 ). Treatment was placed in a confluent pattern of 4–5 curvilinear rows in the temporal juxtapapillary area. The circumferential extent of treatment (ie, number of clock hours) corresponded to the circumferential extent of intraretinal and/or subretinal fluid as determined by contact lens examination and OCT imaging (when available).
Upon completion of the laser treatment, the patient was taken directly to the operating room and underwent pars plana vitrectomy (PPV) with induction of posterior vitreous detachment (PVD), where necessary, using aspiration through the vitreous cutter. No attempt was made to peel anomalous glial tissue from the surface of the pit or internal limiting membrane from the macular area. Fluid-gas exchange with SF 6 or C 3 F 8 gas was performed, with aspiration of fluid immediately anterior to the optic disc in hopes of draining a portion of the subretinal fluid, where present. A drainage retinotomy was employed only in 1 patient with an extensive bullous retinal detachment and in 1 patient with chronic submacular fluid that failed to resolve with the standard procedure. Patients were advised to position face down for 7–10 days postoperatively. Where available, OCT imaging was used to assess the integrity of the intraretinal fluid barrier and the resolution of macular fluid postoperatively. Main outcome measures were change in visual acuity (VA), macular fluid resolution, and recurrence of maculopathy.
Results
Of the 22 patients reviewed, 11 eyes of 11 patients had undergone vitreous surgery at our center and were included in the study. Among the remaining 11 patients, 3 underwent surgery elsewhere and 8 had good VA with mild maculopathy that did not require surgical intervention.
In the study cohort, there were 8 women and 3 men ( Table ). Patients 1, 2, and 5 were included in previous publications. The mean age at onset of symptoms was 33 years (range, 15–65 years) and the mean age at presentation to us was 35 years (range, 16–66 years). Among the 10 eyes without prior vitrectomy on presentation to us, there was complete PVD in 1 eye (10%) (Patient 8) and neither complete nor partial PVD in the remaining 9 eyes (90%). We found no preoperative clinical or OCT evidence for vitreous traction on the optic disc or macula in any eye.
| Patient No. | Age at Presentation/Sex/Eye | Prior Treatment | Presenting VA | Final VA | Procedure(s) | Time From Last Surgery to Final Follow-up (Months) | Time From Last Surgery to Complete Resolution of Fluid (Months) | Recurrence |
|---|---|---|---|---|---|---|---|---|
| 1 | 24/F/OD | N | CF 7′ | 20/100 | PPV, FGx | 143 | 2 | N |
| FLP with PPV, FGx, CE IOL | ||||||||
| FGx followed by FLP | ||||||||
| PPV, FGx, ELP, Cryo, SRF drainage | ||||||||
| 2 | 55/F/OS | FLP x4 | 20/200 | 20/100 | PPV, FGx, ELP | 75 | 1 | N |
| PPV, FGx | PPV with inner retinal fenestration | |||||||
| PPV, FGx, ELP, SRF drainage, CE IOL | ||||||||
| 3 | 32/M/OS | FLP | 20/200 | 20/60 | FLP, PPV, FGx | 4 | 4 | N |
| 4 | 16/F/OD | N | 20/80 | 20/60 | FLP, PPV, FGx | 6 | 6 | N |
| 5 | 34/F/OS | FLP | 20/80 | 20/20 | PPV, FGx, ELP | 95 | 1 | N |
| 6 | 65/F/OS | N | 20/100 | 20/30 | FLP, PPV, FGx, Cryo | 96 | 18 | N |
| 7 | 20/F/OS | FLP x2 | 20/50 | 20/15 | FLP, PPV, MP, FGx | 20 | 15 | N |
| Fenestration | ||||||||
| 8 | 66/M/OD | N | 20/80 | 20/70 | FLP, PPV, FGx | 35 | 17 | N |
| 9 | 16/M/OD | FLP x2 | 20/100 | 20/30 | FLP, PPV, FGx, Cryo | 25 | 10 | N |
| 10 | 24/F/OD | N | 20/100 | 20/80 | FLP, PPV, FGx | 12 | 12 | N |
| 11 | 35/F/OS | N | 20/150 | 20/300 | FLP, PPV, FGx | 19 | 7.5 | Y |
Five eyes had undergone at least 1 previous juxtapapillary laser treatment without vitrectomy, and none had subsequent resolution of the macular fluid. In all 5 of these patients, there was evidence for continued fluid migration from the pit through retinal layers overlying the laser-induced chorioretinal scar. Other prior treatments are listed in the Table .
Nine of the 11 study eyes underwent a single surgery, consisting of carefully titrated juxtapapillary laser photocoagulation followed by vitrectomy and gas tamponade. The remaining 2 eyes required additional procedures to resolve the macular fluid ( Table ). The additional treatments included an unsuccessful inner retinal fenestration and additional sessions of juxtapapillary laser photocoagulation with gas tamponade. Red-wavelength laser was used for juxtapapillary photocoagulation in all eyes. Laser treatment was delivered at the slit lamp in 9 eyes and as intraoperative endolaser photocoagulation in 2 eyes (both of which had undergone extensive juxtapapillary laser treatment in the past) ( Table ). A third eye received supplemental juxtapapillary endolaser treatment during surgical repair of a total bullous recurrent retinal detachment associated with atypical optic disc coloboma (Patient 1).
The mean length of follow-up since the last retinal surgery was 48.2 months (range, 4–143 months). All 11 eyes (100%) had complete resolution of macular fluid, with an average time to complete resolution of 8.5 months (range, 1–18 months). Only 1 of 11 patients (9%) had recurrence of macular fluid, first noted 14 months postoperatively. This patient (Patient 11) declined further surgery, since the postoperative visual improvement had been limited by permanent photoreceptor atrophy from longstanding macular detachment.
The average preoperative VA of 20/125 (logMAR 0.81, standard deviation [SD] = 0.36) improved by nearly 4 lines to an average final VA of 20/57 (logMAR 0.45, SD = 0.37) ( P = .0072). Four of the 11 eyes (36%) had VA of 20/40 or better at last follow-up ( Table ). A central scotoma caused by thermal injury to the papillomacular nerve fiber layer was suspected in only 1 eye that had extensive juxpapillary chorioretinal scarring owing to many prior laser treatments (Patient 2). The VA improved in this eye from 20/200 preoperatively to 20/100 postoperatively. Although formal visual field testing was not performed, no other patients reported new scotomas following laser treatment.
On postoperative OCT images, laser-induced retinal scarring appeared as an area of retinal thinning overlying RPE atrophy and/or hyperplasia ( Figures 2–5 ). Detailed analysis of the juxtapapillary laser scar in the 9 eyes for which postoperative OCT imaging was available revealed thinning and disorganization of all retinal layers external to the inner plexiform layer (4 eyes) or inner nuclear layer (3 eyes). In the remaining 2 eyes (Patients 1 and 2), which had undergone multiple laser procedures including endolaser delivery, the laser scar appeared as an area of marked retinal thinning with no discernible layers. The intraretinal scar was typically “dry” (devoid of intraretinal fluid) on early postoperative images following resolution of the vitreous gas bubble, but intraretinal or subretinal fluid in the macular area often required many additional months to resolve ( Figures 2–5 ). In 4 eyes, OCT imaging showed intraretinal fluid emanating from the cavitary disc lesion that appeared to be blocked by the laser-induced subretinal and intraretinal scar, suggesting an effective fluid barrier ( Figures 2–5 ). In the only eye with recurrent maculopathy, OCT images showed fluid migrating through previously lasered retina, indicating failure to achieve a fluid barrier with a single procedure in this patient ( Figure 6 ).
Selected Cases
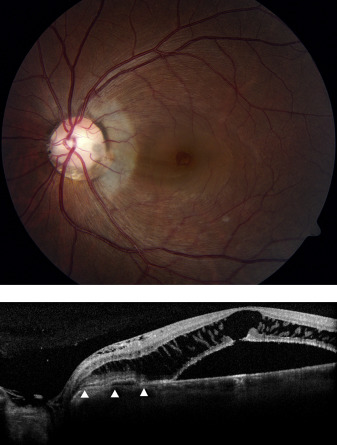
Patient 6
A 65-year-old woman with a diagnosis of primary open-angle glaucoma presented with decreased VA and a circular dark area in the central visual field of the left eye. The VA was 20/100 and slit-lamp biomicroscopy revealed subtle breaks in a diaphanous membrane overlying the optic cup in the left eye. There was serous macular detachment as well as intraretinal fluid both nasal and temporal to the nerve ( Figure 2 , Top). The patient underwent titrated red-wavelength juxtapapillary laser photocoagulation at the slit lamp, followed immediately by pars plana vitrectomy with gas tamponade and face-down positioning for 1 week. The fovea was dry 1 month postoperatively and displaced subretinal fluid in the inferotemporal macula resolved slowly over 18 months. At final follow-up 96 months postoperatively, the VA was 20/30 OS and OCT imaging demonstrated fluid within the optic nerve head cavitation that did not extend beyond the laser-induced retinal fluid barrier ( Figure 2 , Bottom).
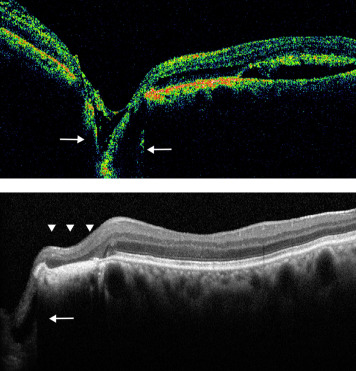
Patient 7
A 20-year-old woman was evaluated for persistent macular fluid in the left eye following 2 laser treatments and a partial-thickness inner retinal fenestration (without vitrectomy). Examination 2 weeks following the fenestration procedure revealed VA of 20/50 OS. Fundus biomicroscopy of the left eye showed a typical optic disc coloboma with diffuse schisis-like thickening of the macula. OCT imaging demonstrated fluid beneath the nerve fiber layer within the disc cavitation that tracked into the retinal stroma throughout the macula despite juxtapapillary laser scarring ( Figure 3 , Top). The patient underwent red-wavelength confluent juxtapapillary laser photocoagulation treatment at the slit lamp, using moderate-intensity burns and avoiding the pigment hyperplasia caused by previous laser treatment. Care was taken to avoid thermal uptake in the inner retina. Immediately thereafter, she was taken to the operating room, where she underwent pars plana vitrectomy with peeling of the posterior hyaloid membrane and fluid-gas exchange with postoperative face-down positioning for 1 week. Slow and complete resolution of intraretinal fluid occurred over approximately 15 months, with improvement of VA to 20/15. Postoperative OCT imaging showed fluid emanating from the disc cavitation that appeared to be blocked by the laser-induced subretinal and intraretinal scar ( Figure 3 , Middle and Bottom).
Patient 8
A 66-year-old man with glaucoma was evaluated for a chronic serous macular detachment in the right eye. The VA was 20/80 OD. Fundus biomicroscopy showed a deeply cupped nerve, with schisis-like intraretinal fluid extending throughout the macula and papillomacular bundle as well as nasal to the optic disc. There was subretinal fluid and subretinal vitelliform material in the central macula ( Figure 4 , Top). At the slit lamp, he underwent juxtapapillary laser photocoagulation using moderate-intensity burns in the deep layers of the retina, attempting to achieve thermal spread into the middle but not the inner retinal layers. He was then immediately taken to the operating room for pars plana vitrectomy and fluid-gas exchange with 8% C 3 F 8 . One month postoperatively, OCT imaging showed a dry, compact laser scar with decreasing intraretinal fluid and persistent chronic subretinal fluid ( Figure 4 , Middle). The macular fluid slowly resolved over 17 months and the macula remained dry 3 years postoperatively, with visual acuity stabilizing at 20/70. OCT imaging 18 months postoperatively ( Figure 4 , Bottom) showed a temporal juxtapapillary laser scar with dry macula but persistent intraretinal fluid nasal to the disc where there was no laser barrier.
Patient 10
A 24-year-old woman was evaluated for progressive central vision loss in the right eye over the previous year. The visual acuity measured 20/100 OD. Fundus biomicroscopy and OCT imaging showed schisis-like intraretinal fluid in the outer macula as well as in the inner retina near the optic disc ( Figure 5 , Top). A large outer foveal defect was present, with preservation of the inner foveal layers. There was glial or condensed vitreous tissue overlying a small pit in the temporal aspect of the optic disc. Juxtapapillary red-wavelength laser photocoagulation was performed at the slit lamp, titrating the burn to moderate intensity and avoiding spread into the nerve fiber layer. This was followed immediately by pars plana vitrectomy with separation of the posterior hyaloid, fluid-gas exchange, and postoperative face-down positioning for 1 week. Six weeks postoperatively, OCT imaging showed a dry laser scar and decreasing intraretinal fluid in the macula ( Figure 5 , Middle). The patient was lost to follow-up until 1 year postoperatively, when the visual acuity had improved to 20/80. Fundus biomicroscopy and OCT imaging showed resolution of all macular fluid and a small residual outer foveal defect ( Figure 5 , Bottom). A small amount of inner retinal fluid emanating from the disc pit did not extend beyond the laser barrier.
Patient 11
A 35-year-old woman diagnosed with optic pit at the age of 9 years reported blurred central vision in the left eye for at least 15 years. The visual acuity measured 20/150 OS. Fundus examination and OCT imaging revealed shallow subretinal fluid throughout the macula and extending beyond the inferior arcade ( Figure 6 , Top). Pigment changes underlying the subretinal fluid and atrophy of photoreceptors seen on OCT imaging reflected the long duration of the macular detachment. She underwent juxtapapillary laser photocoagulation using red-wavelength laser and slit-lamp delivery, with energy titration to produce a moderate-intensity gray-white burn that spared the inner retina. This was followed immediately by pars plana vitrectomy with induction of posterior vitreous detachment and fluid-gas exchange, followed by 1 week of face-down positioning. There was resolution of all subretinal fluid by 7.5 months postoperatively ( Figure 6 , Middle), but visual acuity was unimproved, likely owing to detachment chronicity of 15 years. The patient returned 6 months later with new intraretinal fluid extending from the pit across the laser scar and into the macula. She elected no further intervention, given the limited visual potential. She was last seen 19 months postoperatively, with OCT evidence of further migration of fluid into the subfoveal space ( Figure 6 , Bottom).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


