Chapter 12 Fine-Needle Aspiration of the Thyroid Gland
Introduction
 Please go to expertconsult.com to view related videos Thyroid Nodule Fine-Needle Aspiration Techniques and Preparation of Thyroid Fine-Needle Aspiration Slides.
Please go to expertconsult.com to view related videos Thyroid Nodule Fine-Needle Aspiration Techniques and Preparation of Thyroid Fine-Needle Aspiration Slides.
Fine-needle aspiration (FNA) is the crucial diagnostic test for evaluating the patient with a thyroid nodule. The result of the FNA determines in large part whether a patient can be followed clinically or referred for surgery. Guidelines have been established for selecting those nodules that need aspiration1,2 (see Chapter 11, The Evaluation and Management of Thyroid Nodules).
Once the decision has been made to perform an FNA, attention to technical details can improve results: in general, smaller needles (25 and 27 G) are superior to larger ones; a shorter “dwell time” (the time the needle is kept in the lesion) is often superior to longer dwell times, which introduce more blood; and rapid oscillations within the nodule (two to five per second) are better than slow excursions. Communication between the operator (if the FNA is not performed by a pathologist) and the pathologist is essential. The pathologist’s interpretation is greatly aided if essential clinical information (e.g., history of hypothyroidism, etc.) is provided on the requisition form. Although reporting terminology has been nonstandard and confusing in the past, a new reporting framework called The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) consists of six general diagnostic categories and promises to standardize the reporting of thyroid FNA results.3–5
Indications for Thyroid FNA
Thyroid nodules are typically discovered either by palpation or through an imaging study. A palpable thyroid nodule should undergo further evaluation to determine if an FNA is warranted.1,2,6 Before the decision is made, a serum thyrotropin level (TSH) and thyroid ultrasound (US) should be obtained.2,6–9 Patients with a normal or elevated serum TSH level should proceed to a thyroid US to determine if an FNA needs to be performed. Those with a depressed serum TSH should have a radionuclide thyroid scan, the results of which should be correlated with the sonographic findings.2,6,8–10 Functioning thyroid nodules in the absence of significant clinical findings do not require an FNA because the incidence of malignancy is exceedingly low.11 A nodule that appears either iso- or hypofunctioning on radionuclide scan should be considered for FNA based on the US findings (see Chapter 11, The Evaluation and Management of Thyroid Nodules).2,6
Thyroid nodules with a maximum diameter greater than 1 to 1.5 cm on US should be considered for biopsy unless they are simple cysts or septated cysts with no solid elements. FNA may also occasionally be replaced by periodic follow-up for nodules of borderline size (between 1 to 1.5 cm in maximum diameter) if they have sonographic features that are strongly associated with benign cytology (see Chapter 11, The Evaluation and Management of Thyroid Nodules).1
Subcentimeter nodules with sonographically suspicious features can also be considered for FNA according to guidelines of the American Thyroid Association,2 the Academy of Clinical Thyroidologists,12 and a collaborative effort of the American Association of Clinical Endocrinologists and the Associazione Medici Endocrinologi.1,24,25 Sonographically suspicious features include microcalcifications, hypoechoic solid nodules, irregular/lobulated margins, intranodular vascularity, and nodal metastases (or signs of extracapsular spread) (see Chapter 13, Ultrasound of the Thyroid and Parathyroid Glands). This recommendation is somewhat controversial because it results in the diagnosis of patients with papillary microcarcinomas, in whom a survival benefit following an FNA diagnosis has not been documented. The natural history of such papillary microcarcinomas is not well understood. Most remain indolent, as implied by the 13% prevalence of papillary microcarcinomas in the United States at autopsy examination.26 A minority follow a more aggressive course; this subgroup might be identified by sonographic evidence of lateral cervical node metastases, tumor multifocality, extrathyroidal invasion, or cytopathologic features that suggest a high-grade malignancy27 (see Chapters 18, Papillary Thyroid Cancer, and 19, Papillary Thyroid Microcarcinoma).
Incidental thyroid nodules (“incidentalomas”) may be detected by a variety of imaging modalities, including 18FDG-PET, sestamibi, computed tomography (CT), and magnetic resonance imaging (MRI) scans. Depending on the exact method of detection and size, these incidentalomas can be associated with a cancer risk of approximately 10% to 15% (0% to 29%,)1,12–23 and patients should undergo dedicated thyroid sonographic evaluation. Incidentalomas detected by 18FDG-PET (2% to 3% of all PET scans) have a higher risk of cancer (14% to 50%).2,28–36 A focally 18FDG-PET-avid thyroid nodule is much more likely to be a primary thyroid cancer than metastatic disease to the thyroid, even in patients with an extrathyroidal malignancy. Therefore, a focal nodule that is 18FDG-PET-avid is a clear-cut indication for FNA. Diffuse increased uptake on 18FDG-PET does not warrant FNA unless thyroid sonography detects a discrete nodule. Thyroid incidentalomas detected on sestamibi scans also have a high risk of cancer (22% to 66%),37–41 and therefore all focal hot nodules detected on sestamibi scans that are confirmed by US to be a discrete nodule should undergo FNA.
There are few direct data on the cancer risk of thyroid incidentalomas detected by CT or MRI. Nodules are seen in at least 16% of patients evaluated by neck CT or MRI.42 The risk of cancer in one study was predicted at 10%, but it included only a limited number of patients who were evaluated with FNA.43 CT and MRI features cannot determine the risk of malignancy except in very advanced cases. Until more data are available, incidentalomas seen on CT or MRI should undergo dedicated thyroid sonographic evaluation.
FNA Technique
The fine-needle aspiration (FNA) biopsy was introduced for the first time in the United States in the 1930s, but only during the 1950s in Sweden was widely appreciated as a diagnostic tool. Since then this method has spread worldwide because of its simplicity, safety, and the possibility of repetition.44,45 FNA is regarded as the most accurate method for the selection of patients with thyroid nodules and a very cost-effective diagnostic test.46
The FNA of a thyroid nodule is preferably carried out under sonographic guidance, although when easily palpable, the maneuver can be performed under manual guidance.47 While all nodules larger than 1 cm in a multinodular goiter can be considered for aspiration, often the nodules are selected by the sonographer based on their US appearance. As noted above, sonographically suspicious features include microcalcifications, hypoechoic solid nodules, irregular/lobulated margins, intranodular vascularity, and nodal metastases (or signs of extracapsular spread). A hypoechoic solid pattern with irregular margins and the presence of intralesional calcium deposits are the most important clues for suspecting a malignant lesion.48 The aspiration is performed with thin needles (gauge ranging from 27 G to 20 G). Given that thyroid lesions are usually richly vascularized, it is typically better to use very thin needles (either 27 G or 25 G) rather than larger ones (23 G to 20 G). After applying superficial anesthesia, which may be carried out by spraying the skin with ethyl chloride or by injecting lidocaine subcutaneously, the operator holds the sonographic probe with one hand and performs the aspiration with the other, typically with a syringe-holding pistol. An FNA may also be carried out by simply moving the needle, without any connection to a suction device. In this technique, termed the cytopuncture technique, the cytologic material is extruded from the lesion by capillary action.44,45,49,50 The risk of complications is low (discussed later) even when the number of FNA passes is up to five for each nodule. The procedure can be repeated safely when the smear shows low cellularity at the onsite assessment and a reliable diagnosis cannot be rendered.51 When an onsite assessment of specimen adequacy is available, two passes are usually sufficient.52 However, when an onsite evaluation is not possible or when liquid-based cytology is chosen (discussed later), three to five passes might be required depending on the skill of the operator and the characteristics of the lesion. Once the needle is withdrawn from the lesion, the material is extruded onto glass slides and the smear is fixed with 95% ethyl alcohol for Papanicolaou staining. Alternatively, the smear may be air dried and then stained with May-Grunwald Giemsa, which also gives excellent results in thyroid cytology.
The core-needle biopsy (CNB) procedure involves the use of large-gauge needles (14 G to 19 G). The advantages of this technique in combination with FNA include an increased amount of tissue, which may decrease the number of nondiagnostic samples and provides material for application of ancillary studies. The disadvantages of CNB include the increased possibility of complications, such as hemorrhage and local pain, and the difficulty in performing multiple samplings of the lesion.53,54 Given the potential for CNB-associated pain and complications, we feel the role of CNB should be limited to occasional use in patients with multiple nondiagnostic FNAs who are adverse to diagnostic lobectomy or for tumor subtyping in selected patients with initial FNA data suggesting thyroid lymphoma.
Liquid-based cytology (LBC) techniques represent an alternative slide preparation method to conventional smearing (CS) slide preparation for thyroid cytology. LBC techniques, originally developed for application to gynecologic cervical specimens, have gained widespread acceptance after being applied to both nongynecologic and fine-needle aspiration cytology. This method is based on a two-step procedure: (1) the fixation of the entire specimen in an alcohol-based solution (methanol or ethanol depending on the technique, discussed later) and (2) the automated processing of the material to obtain a thin layer of representative cells. LBC uses a computer-assisted device that allows the transfer of the fixed and partially disaggregated cells onto a single slide. The two most common methods for processing the cytologic samples use an alcohol-based fixative solution. In the first (ThinPrep2000, Hologic Co., Marlborough, Massachusetts), the cells are aspirated from a methanol-based solution (Cytolit) then filtered and transferred onto a positively charged slide. In the second, the cells are collected in an ethanol-based solution (CytoRich), centrifuged twice, then slowly sedimentated onto a poly-L-lysinated slide and eventually stained with a specific hematoxylin-eosin stain (PrepStain LBC, once AutoCyte PREP, TriPath Imaging, Burlington, Vermont). The final result for both methods is one slide for each lesion where all cells are concentrated in a thin layer on the central area of the slide measuring 20 square mm for ThinPrep and 13 square mm for PrepStain LBC.55–60
There is no agreement in the literature as to whether the pathologist should perform the FNA.44,49 If the pathologist performs the aspiration, an immediate evaluation of the sample adequacy is possible. Although clinicians are more familiar with the clinical aspects of the case, there are variable nondiagnostic rates in clinician-performed FNA studies. Experience is an essential requisite to obtain an adequate cytologic sample regardless of the subspecialty of the operator. The procedure should be carried out with appropriate frequency (at least 100 FNAs/year) to maintain competency.61,62
Accuracy of Thyroid FNA
Thyroid FNA is widely accepted as a highly cost-effective and accurate means of evaluating a thyroid nodule. For the diagnosis of papillary carcinoma, thyroid FNA is considered by many to be at least as accurate as frozen section reflecting the importance of nuclear cytology for diagnosing papillary carcinoma.63 False-negative and false-positive thyroid FNA diagnoses occur, but they are uncommon, averaging less than 5% and 1%, respectively.64 Such errors are a result of both sampling errors as well as errors in interpretation. In experienced hands, the diagnostic accuracy of thyroid FNA for technically satisfactory specimens is greater than 95%, with positive predictive values of 89% to 98% and negative predictive values of 94% to 99%.65,66 These values, however, are dependent on how the “atypia of undetermined significance/follicular neoplasm of undetermined significance” and “suspicious for a follicular neoplasm” categories are used in the calculations.67 Sensitivities for thyroid FNA range from 43% to 98%, and specificities range from 72% to 100%. These wide ranges in part also reflects the skill of the person performing the FNA as well as the expertise of the cytopathologist interpreting the specimens. For the evaluation of cystic thyroid lesions, FNA is reported to have a low sensitivity (40%), as cystic aspirates will often yield cyst contents only (foam cells, hemosiderin-laden macrophages, and acellular debris) with rare epithelial cells. Caution is warranted in interpreting cystic thyroid aspirates with limited cellularity, as a subset of thyroid cysts represent cystic papillary carcinomas.
Reporting Terminology: The Bethesda System
It is critical that the pathologist communicate thyroid FNA interpretations in terms that are succinct, unambiguous, and clinically helpful. Historically, terminology for thyroid FNA has varied from one laboratory to another, creating confusion and hindering the sharing of clinically meaningful data among multiple institutions. The 2007 National Cancer Institute (NCI) Thyroid Fine Needle Aspiration FNA State of the Science Conference acknowledged the importance of developing a uniform terminology for reporting thyroid FNA results. The discussions and conclusions regarding terminology and morphologic criteria from the NCI meeting3,68 form the framework for this terminology, called The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC).4,5
For clarity of communication, TBSRTC recommends that each report begin with one of six general diagnostic categories (Table 12-1). For some categories, TBSRTC offers a choice of two names; a consensus was not reached at the NCI conference on a single name for these categories. Each of the categories has an implied cancer risk that links it to an evidence-based management guideline (Table 12-2). The term indeterminate is not advised for reporting thyroid FNA results because its meaning is not sufficiently specific and its use has been highly variable.
Table 12-1 The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC)
| I. Nondiagnostic or Unsatisfactory |
| II. Benign |
| III. Atypia of Undetermined Significance or Follicular Lesion of Undetermined Significance |
| IV. Follicular Neoplasm or Suspicious for a Follicular Neoplasm |
| V. Suspicious for Malignancy |
| VI. Malignant |
From Ali SZ, Cibas ES: The Bethesda System for Thyroid Cytopathology: definitions, criteria, and explanatory notes, New York, 2009, Springer. With kind permission of Springer Science and Business Media.
Table 12-2 The Bethesda System for Reporting Thyroid Cytopathology: Implied Risk of Malignancy and Recommended Clinical Management
| Diagnostic Category | Risk of Malignancy (%) | Usual Management* |
|---|---|---|
| Nondiagnostic or unsatisfactory | 1-4 | Repeat FNA with ultrasound guidance |
| Benign | 0-3 | Clinical follow-up |
| Atypia of undetermined significance or follicular lesion of undetermined significance | ~5-15† | Repeat FNA |
| Follicular neoplasm or suspicious for a follicular neoplasm | 15-30 | Lobectomy |
| Suspicious for malignancy | 60-75 | Near-total thyroidectomy or surgical lobectomy‡ |
| Malignant | 97-99 | Near-total thyroidectomy‡ |
* Actual management may depend on other factors (e.g., clinical, sonographic) besides the FNA interpretation.
† Estimate extrapolated from histopathologic data from patients with “repeated atypicals.” Yang J, Schnadig V, Logrono R: Fine-needle aspiration of thyroid nodules: a study of 4703 patients with histologic and clinical correlations. Cancer 111:306-315, 2007; Yassa L, Cibas ES, Benson CB, et al: Long-term assessment of a multidisciplinary approach to thyroid nodule diagnostic evaluation. Cancer 111:508-516, 2007.
‡ In the case of “suspicious for metastatic tumor” or a “malignant” interpretation indicating metastatic tumor rather than a primary thyroid malignancy, surgery may not be indicated.
Modified from Ali SZ, Cibas ES: The Bethesda System for Thyroid Cytopathology: definitions, criteria, and explanatory notes, New York, 2009, Springer. With kind permission of Springer Science and Business Media.
For some of the general categories, subcategorization can be informative and is often appropriate; recommended terminology is shown in Table 12-1. Additional descriptive comments beyond such subcategorization are optional and left to the discretion of the cytopathologist. Each of the six categories is discussed in greater detail in the sections that follow.
Nondiagnostic Thyroid Aspirates
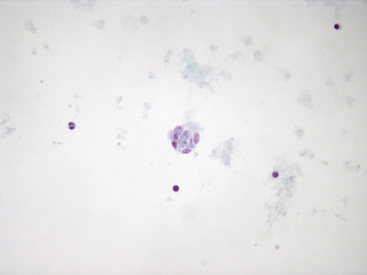
The cytopathologist must receive an adequate biopsy specimen in order to make a meaningful and accurate cytopathologic evaluation. The final cytologic specimen must be adequate in terms of both cellularity and quality (thickness, fixation, and staining). Approximately 10% to 20% of thyroid aspirates are “nondiagnostic.” Both operators and patients should be aware that an FNA does not always yield a diagnostic result. Nondiagnostic samples may occur for two reasons: (1) the sampling of the lesion yields material unsatisfactory for a definitive diagnosis or (2) the aspirated material is nonrepresentative. FNA material is defined as unsatisfactory when fixation, smearing, or staining artifacts impair the interpretation of the final slide (Figure 12-1).69 A slide is nonrepresentative when the cellularity does not represent the true components of the lesion (e.g., insufficient amount of follicular cells).3,68,70 In both standard cytology slide preparation and LBC, the adequacy criteria are met when at least six clusters of 10 to 20 well-preserved cells are observed.3,68,70–73 Discrete colloid on a smear does not necessarily mean the lesion is a benign nodule unless the amount of the follicular component is adequate.
Among the nondiagnostic samples that are nonrepresentative, cystic lesions are the most frequently encountered.74 Thyroid cysts may contain solid areas detectable at the sonographic examination. In this instance, such solid areas should be specifically sampled to optimize the sample’s cellularity. Such optimization is not always possible. In such cases, cytologic reporting of certain cystic colloid nodule lesions represent an exception to the above noted cytologic adequacy rule where FNA shows abundant colloid and very few fragmented macrofollicles. These cases are often signed out as “Benign—abundant colloid, consistent with a colloid nodule.” Care should be taken to carefully observe the few follicular cells present to exclude the unlikely possibility of a macrofollicular cystic variant of papillary thyroid carcinoma. If the cystic cytologic result is nondiagnostic, repeat FNA and careful US follow-up should be planned (within 6 to 18 months according to different guidelines).2,75 When an FNA of a cystic nodule with a solid component is repeatedly nonrepresentative, the surgical excision of the nodule may be considered because between 8% and 19% of such cases are malignant.50,56,71,74



