Purpose
To evaluate the increase in tear fluid volume induced by 3% diquafosol ophthalmic solution in normal human eyes.
Design
Prospective, randomized, double-masked, comparative study.
Methods
Twenty healthy adults (17 males and 3 females; mean age, 38.8 years) underwent topical instillation of 2 ophthalmic solutions, artificial tears in 1 eye and 3% diquafosol ophthalmic solution in the fellow eye, in a masked manner. The radius of curvature of the central lower tear meniscus was measured at 5, 10, 15, 30, and 60 minutes after instillation by use of reflective meniscometry, and subjects’ self-evaluated symptoms of wetness and stinging using a visual analog scale.
Results
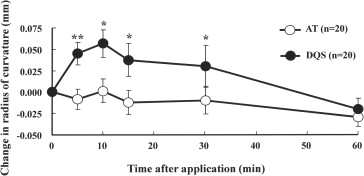
Changes after instillation in the radius of curvature from baseline (artificial tear group vs diquafosol group; mean ± standard error of the mean) were as follows: at 5 minutes, −0.008 ± 0.012 vs 0.045 ± 0.013; at 10 minutes, 0.001 ± 0.014 vs 0.057 ± 0.016; at 15 minutes, −0.012 ± 0.014 vs 0.037 ± 0.019; at 30 minutes, −0.010 ± 0.016 vs 0.030 ± 0.025; and at 60 minutes, −0.029 ± 0.012 vs −0.020 ± 0.012. The diquafosol group showed significantly greater values from 5 to 30 minutes after instillation. Of the 40 eyes, 13 showed abnormal tear film breakup time (≤5 seconds). The diquafosol group had significantly more wetness at 15 minutes after instillation than did the artificial tear group.
Conclusions
Topical instillation of 3% diquafosol ophthalmic solution increases tear fluid on the ocular surface for up to 30 minutes in normal human eyes.
According to the Dry Eye Workshop and Dry Eye Society of Japan, dry eye is “a multifactorial chronic disease of the tears and keratoconjunctival epithelium, accompanied by eye symptoms and visual disturbance.” Therefore, dry eye can be described as a disease in which various risk factors trigger a vicious circle that disrupts the normal healthy state between the tear film and ocular surface epithelium, ultimately causing various symptoms summarized as unidentified ocular complaints. Dry eye involves various intrinsic and extrinsic factors and is categorized into aqueous deficient dry eye caused by Sjögren syndrome (SS) and lacrimal deficiency and evaporative dry eye caused by meibomian gland dysfunction, visual display terminal work, low temperature or low humidity, and contact lens wear. In recent years, epidemiologic studies on dry eye have been conducted worldwide, and dry eye is now recognized as a common eye disease that affects the quality of life and requires improved treatment methods.
In Japan, ocular local treatment with ophthalmic solutions such as artificial tears, sodium hyaluronate, soft steroids, autologous serum, or punctal plugs has been the main treatment regimen against dry eye symptoms such as tear film instability, ocular surface inflammation, and epithelial disorders. The tear film consists of lipids, water, and secreted mucin. The secretory mucin component is distributed spatially in tear film and declines in concentration from the epithelium toward the lipid layer. It improves stability of the entire tear film by reducing the surface tension. Therefore, decreased mucin in the tear reduces tear film stability, which is a causal factor for dry eye. Recently, an ophthalmic solution that can promote mucin and fluid secretion, 3% diquafosol ophthalmic solution (Diquas ophthalmic solution 3%; Santen Pharmaceutical Co, Ltd, Osaka, Japan), and an ophthalmic solution that promotes mucin production, 2% rebamipide ophthalmic suspension (Mucosta ophthalmic suspension UD2%; Otsuka Pharmaceutical Co., Ltd., Tokyo, Japan), have become available as prescription drugs. Both are potentially more effective treatments for dry eye than previous artificial tear formulations.
Diquafosol ophthalmic solution was introduced exclusively in Japan in December 2010. It contains diquafosol sodium, a P2Y 2 receptor agonist, as the active ingredient. The P2Y 2 receptor is distributed widely in the body, and its endogenous agonists are adenosine triphosphate (ATP) or uridine triphosphate (UTP). At the ocular surface, it is expressed in the cornea, conjunctiva including goblet cells, and meibomian gland, and it has been reported that ATP and UTP promote fluid and mucin secretion in the conjunctival tissue. Diquafosol sodium is a dinucleotide derivative and exhibits P2Y 2 receptor agonist activity. In the conjunctival epithelium, diquafosol sodium accelerates fluid transport from the serosal to mucosal (tear) side via chloride channel activation after intracellular calcium ion concentration elevation. Moreover, diquafosol sodium reportedly facilitates the secretion of soluble mucin from conjunctival goblet cells and stimulates the expression of membrane-associated mucin on the corneal epithelium. These actions of diquafosol ophthalmic solution thereby stabilize the tear film on the ocular surface and provide therapeutic relief for dry eye. Several clinical studies have demonstrated the superior effect of 3% diquafosol ophthalmic solution for the treatment of dry eye ; however, water and mucin secretion facilitated by diquafosol sodium has been confirmed only in in vitro models and in in vivo rabbit, cat, and rat models.
Reflective meniscometry is a specialized assessment method for measuring the radius value of the tear meniscus. We previously reported a linear relationship between curvature radius of tear meniscus and the cumulative tear volume, indicating that radius of tear meniscus curvature is useful to monitor the time-dependent changes in the tear volume on the ocular surface after the topical instillation of eye drops.
The purpose of the present study was to focus on the effect of 3% diquafosol ophthalmic solution as an aqueous enhancer by use of reflective meniscometry, a noninvasive method to measure the tear volume, to evaluate changes in the ocular surface fluid volume induced by diquafosol ophthalmic solution in healthy human eyes.
Methods
Approval was obtained from the Institutional Review Board of Kyoto Prefectural University of Medicine, Kyoto, Japan, before the initiation of the study. The research was conducted in compliance with the Declaration of Helsinki, and prior written informed consent was obtained from all subjects after explanation of the nature of the study and possible consequences associated with participation in the study.
Twenty healthy subjects (40 eyes) were enrolled in this randomized, treatment-masked, bilateral eye comparison study (17 males and 3 females; age range, 26 to 50 years; mean age, 38.8 ± 6.9 years). The following baseline dry eye screening examinations were conducted: fluorescein staining of the cornea and conjunctiva (scored from 0 to 9 in accordance with the van Bijesterveld scheme), a 5-minute Schirmer I test (no anesthesia used), a series of 3 fluorescein tear film breakup time (BUT) measurements (mean value reported), and periodic questioning of the subject regarding self-described dry eye symptoms. Subjects were considered ineligible if they met at least 2 of the following criteria in both eyes: (1) total corneal and conjunctival fluorescein staining scores of 3 or more, (2) Schirmer I test results of 5 mm or less or TBUT of 5 seconds or less, and (3) dry eye symptoms based on Japanese dry eye diagnostic criteria.
All 20 subjects received a single drop of 3% diquafosol ophthalmic solution in 1 eye and a single drop of artificial tear (Soft Santear; Santen Pharmaceutical Co., Ltd.) in the fellow eye. Those 2 ophthalmic solutions were assigned randomly to the right or left eye for each subject, and investigators remained masked and treatment of each subject’s eyes remained unidentified throughout the study. The radius of curvature of the central lower tear meniscus was measured by video meniscometry as an index of the total tear fluid volume over the ocular surface. In video meniscometry, white light is projected from the video meniscometer onto the central lower tear meniscus through a target comprising a series of horizontal stripes, and the specular reflex image of the target is recorded using a digital video recorder. Image analysis software was used to calculate the radius of tear meniscus curvature by application of the concave mirror formula. Recordings of the target image were acquired at baseline (before instillation) and 5, 10, 15, 30, and 60 minutes after instillation of a single eye drop. In addition, ocular symptoms (ie, wetness or stinging) also were recorded by the subjects using a 100-mm visual analog scale (VAS). The calculated radius of curvature and subjective ocular symptom levels were compared with baseline values at each assessment time point for both eyes treated with diquafosol ophthalmic solution and eyes treated with artificial tears. The maximum change in radius value of tear meniscus curvature (maximum change in radius value of curvature = maximum radius value of curvature − baseline radius value of curvature [mm]) was calculated for each individual eye. The area under the curve (AUC (0–60) ; mm × minutes), an indicator of tear retention on the ocular surface, was calculated using the mean change in radius values of curvature curve from 0 to 60 minutes according to the trapezoidal rule.
Statistical Analysis
Paired t tests were used for statistical comparison between the diquafosol ophthalmic solution and artificial tear groups. The Pearson correlation coefficient was used to assess the relationship between the maximum change in radius value and baseline Schirmer I test value. A P value of less than .05 was considered statistically significant.
Results
The baseline ocular signs were not significantly different between the eyes treated with diquafosol ophthalmic solution and those treated with artificial tears ( Table ), and no subject experienced dry eye symptoms. The mean radius values at baseline were 0.306 ± 0.017 for the diquafosol ophthalmic solution group and 0.296 ± 0.020 for the artificial tear group (no significant difference by paired t test).
| AT Group (n = 20 Eyes) | DQS Group (n = 20 Eyes) | |
|---|---|---|
| Fluorescein score (0 to 9 points) | 0.40 ± 0.20 | 0.15 ± 0.10 |
| Fluorescein TBUT (0 to 10 seconds) | 7.0 ± 0.8 | 7.4 ± 0.9 |
| Schirmer test (0 to 35 mm) | 21.3 ± 2.5 | 24.0 ± 2.7 |
| Baseline R values (mm) | 0.296 ± 0.020 | 0.306 ± 0.017 |
| Ocular wetness (0 to 100 mm) | 9.9 ± 3.9 | 11.8 ± 4.2 |
| Ocular stinging (0 to 100 mm) | 2.8 ± 1.3 | 1.9 ± 1.0 |
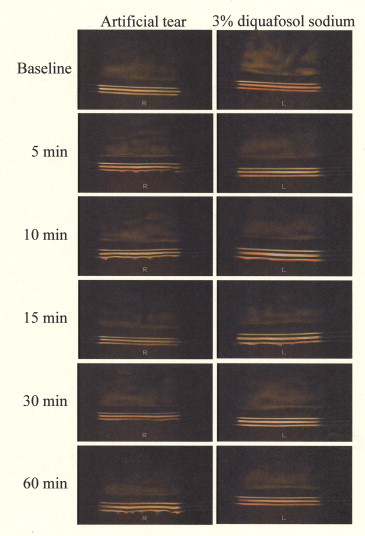
Representative changes in the meniscus image after instillation of each eye drop are shown in Figure 1 , and time-dependent changes in radius values of tear meniscus curvature are plotted in Figure 2 . The mean change in radius values in the artificial tear group were −0.008 ± 0.012, 0.001 ± 0.014, −0.012 ± 0.014, −0.010 ± 0.016, and −0.029 ± 0.012 at 5, 10, 15, 30, and 60 minutes after instillation, respectively, showing no apparent changes in the radius value. In contrast, the mean change in radius values in the diquafosol ophthalmic solution group were 0.045 ± 0.013, 0.057 ± 0.016, 0.037 ± 0.019, 0.030 ± 0.025, and −0.020 ± 0.012, at 5, 10, 15, 30, and 60 minutes after instillation, respectively. Diquafosol ophthalmic solution increased the radius value of tear meniscus curvature from 5 to 30 minutes after instillation, and the effect was significant compared with that of artificial tears ( P < .05, time-matched paired t test).
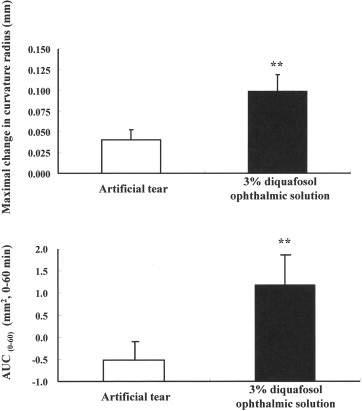
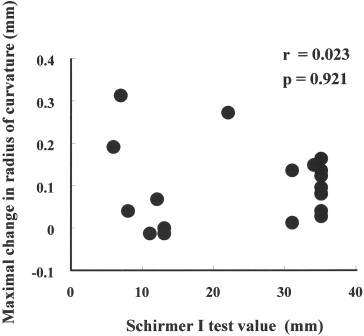
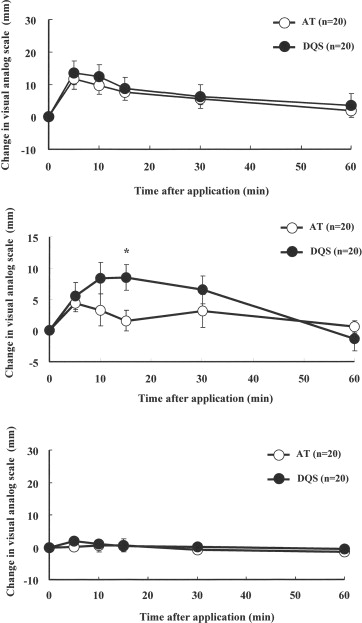
The mean maximum change in radius value and the mean AUC (0–60) in the eyes treated with diquafosol ophthalmic solution were significantly higher than those in the eyes treated with artificial tears (maximal change in radius value, 0.099 ± 0.020 vs 0.040 ± 0.012; P = .0055, paired t test; AUC (0–60) , 1.184 vs −0.520; Figure 3 ). No significant correlation was found between the maximum change in radius value of tear meniscus curvature and baseline Schirmer I test values ( R = 0.023; Figure 4 ). Time-dependent changes in ocular symptoms (ie, wetness or stinging) as measured by VAS scores are shown in Figure 5 . Although the VAS scores for wetness increased in both the diquafosol ophthalmic solution and artificial tears groups, there was no significant difference between the 2 groups at any time point ( Figure 5 , Top). However, in eyes with abnormal TBUT (≤5 seconds), subjects reported significantly higher VAS wetness scores for the diquafosol ophthalmic solution-treated eye ( P = .024, time-matched paired t test; Figure 5 , Middle). Neither eye drop formulation caused stinging, as indicated by the VAS scores ( Figure 5 , Bottom).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


