Facial Reanimation
Tessa A. Hadlock
Rehabilitation of the paralyzed face remains a challenging problem for otolaryngologists, and its proper management may require input from facial plastic surgeons, head and neck reconstruction specialists, otologists, and adjunct medical personnel. Following viral nerve insult, traumatic nerve injury, or intentional sacrifice with repair or cable grafting, regenerative results vary greatly and can lead to hypofunction, hyperfunction, aberrant regeneration, or a combination of these phenomena. The functional problems related to facial paralysis are extensive. In the upper face, they include brow ptosis, leading to a visual field deficit and hygiene issues related to skin desquamation onto the cornea. In addition, loss of a blink reflex leads to corneal exposure of the affected eye, there is lacrimal gland hypo- or hyperfunction, and lower lid paralysis results in ectropion as well as poor lacrimal punctal function. In the central zone of the face, patients may suffer with unilateral nasal obstruction, upper lip ptosis, lack of oral commissure excursion with smiling, oral incompetence to both liquids and solids, and articulation problems. In the lower face, lower lip weakness also contributes to oral incompetence, and platysmal synkinesis can restrict smiling and lead to superficial torticollis symptoms. Facial paralysis also has a significant impact on nonverbal communication, and the loss of one’s ability to express positive emotions on the face rivals the above-listed issues as the most dominant source of patient devastation.
Herein, we review the management of facial nerve deficits and describe the surgical management of each distinct zone of the paralyzed face, with regard to recovery potential, prognosis, and patient factors that contribute to surgical decision making. We emphasize the systematic assessment of each facial zone as a critical step to ensure comprehensive management of the paralyzed face (1).
NERVE REPAIR AND GRAFTING
Nerve Injury Classification
Nerve injuries are classified according to the level of microanatomical disruption. According to the Sunderland classification system (2), level 1 injury has no microanatomic disruption but a simple temporary dysfunction of the membrane sodium channels, resulting in transient inability of the nerve to transmit impulses. In level 2 injury, axons are disrupted, though their individual endoneurial channels are not, so that when regeneration occurs, there is little to no axonal misrouting. In level 3 injury, endoneurial sheaths are violated, though perineurium is left intact. Recovery from this type of injury occurs over months and inevitably results in some synkinesis. Level 4 injury implies total perineurial disruption, where only the outer epineurial sheath is intact, and spontaneous recovery is generally poor. Level 5 injury refers to total anatomic disruption, including the epineurium. No spontaneous recovery is expected from this injury without surgical intervention.
Management of Neural Discontinuity
In cases of complete facial nerve disruption, reestablishment of direct nerve continuity is required for restoration of muscle function. Reapproximation of freshened edges must be accomplished without placing tension across the suture line, through simple epineurial sutures. When injury occurs within the temporal bone, thorough exposure of the site of injury is recommended, and surgical repair is indicated when 50% of the diameter of the facial nerve appears to have been violated (3).
After facial nerve injury or sacrifice, if a tensionless neurorrhaphy is not possible because of a gap between the cut edges, then a nerve graft is employed to bridge the
neural defect. In facial nerve reconstruction, the three most commonly employed nerve grafts are the great auricular nerve, the sural nerve, and the medial antebrachial cutaneous nerve (Fig. 178.1). For short nerve gaps in the absence of head and neck malignancy, the great auricular nerve is a convenient choice. This often does not require a separate incision from the primary facial nerve exposure incision. The resulting anesthesia to the ipsilateral auricle is well tolerated, and the nerve is of adequate diameter and caliber to provide a suitable graft. However, for nerve gaps of greater than 10 cm, the great auricular nerve does not always provide sufficient length, and the sural nerve becomes a better option. The nerve is removed from the leg via a short incision adjacent to the lateral malleolus and can be harvested through a series of stair-step incisions, a minimally invasive stripping technique, using endoscopic equipment (Fig. 178.2). The resulting segment of anesthetic skin on the dorsum of the foot does not pose a significant clinical problem, and the nerve can yield up to 30 cm in length. For total facial nerve reconstruction from the main trunk to the peripheral branches, the medial antebrachial cutaneous nerve is most appropriate. There are at least four reliable branches, and it provides adequate length to graft the entire facial nerve, from the geniculate ganglion to the medial border of the parotid gland.
neural defect. In facial nerve reconstruction, the three most commonly employed nerve grafts are the great auricular nerve, the sural nerve, and the medial antebrachial cutaneous nerve (Fig. 178.1). For short nerve gaps in the absence of head and neck malignancy, the great auricular nerve is a convenient choice. This often does not require a separate incision from the primary facial nerve exposure incision. The resulting anesthesia to the ipsilateral auricle is well tolerated, and the nerve is of adequate diameter and caliber to provide a suitable graft. However, for nerve gaps of greater than 10 cm, the great auricular nerve does not always provide sufficient length, and the sural nerve becomes a better option. The nerve is removed from the leg via a short incision adjacent to the lateral malleolus and can be harvested through a series of stair-step incisions, a minimally invasive stripping technique, using endoscopic equipment (Fig. 178.2). The resulting segment of anesthetic skin on the dorsum of the foot does not pose a significant clinical problem, and the nerve can yield up to 30 cm in length. For total facial nerve reconstruction from the main trunk to the peripheral branches, the medial antebrachial cutaneous nerve is most appropriate. There are at least four reliable branches, and it provides adequate length to graft the entire facial nerve, from the geniculate ganglion to the medial border of the parotid gland.
 Figure 178.1 Common donor nerves in facial nerve reconstruction. A: Great auricular nerve. B: Sural nerve. C: Medial antebrachial cutaneous nerve. |
For both primary nerve repair and nerve grafting, surgery should be performed within the first 72 hours after injury or sacrifice, irrespective of the need for subsequent
radiation therapy (4). During this time frame, the distal nerve segments retain electrical stimulability, making identification easier. Meticulous debridement and careful microsurgical technique are of paramount importance in optimizing outcome. There is debate as to the best method of nerve coaptation, as it applies to both primary and graft repair. Epineurial repair has been contrasted to fascicular repair, though no study has convincingly demonstrated improved regenerative outcome based upon fascicular facial nerve repair. Therefore, given its relative simplicity, the current standard is to perform epineurial suture repair. Though not fully established as more efficacious, it is now becoming commonplace to further reinforce the repair using fibrin glue stabilization (5).
radiation therapy (4). During this time frame, the distal nerve segments retain electrical stimulability, making identification easier. Meticulous debridement and careful microsurgical technique are of paramount importance in optimizing outcome. There is debate as to the best method of nerve coaptation, as it applies to both primary and graft repair. Epineurial repair has been contrasted to fascicular repair, though no study has convincingly demonstrated improved regenerative outcome based upon fascicular facial nerve repair. Therefore, given its relative simplicity, the current standard is to perform epineurial suture repair. Though not fully established as more efficacious, it is now becoming commonplace to further reinforce the repair using fibrin glue stabilization (5).
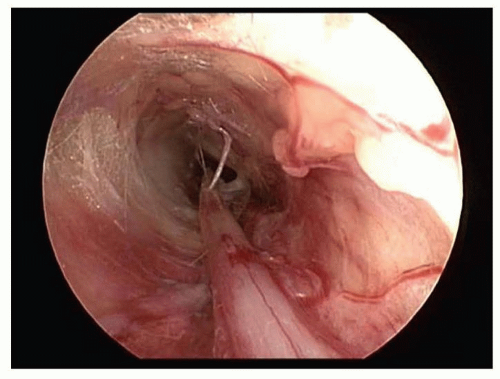 Figure 178.2 Endoscopic view of sural nerve during harvest. Note the nerve at the 6 o’clock position. |
Reinnervation Techniques
When the reestablishment of neural continuity is not possible based upon absence of an adequate proximal facial nerve stump at the brainstem, or severe comminution within the temporal bone, an alternative approach to restoring neural input to the facial musculature involves nerve substitution. This approach, also termed reinnervation, involves performing surgery to deliver neural input to the distal facial nerve and musculature via an alternative motor nerve. The hypoglossal facial transfer is most often used, though investigators have studied the utility of the spinal accessory nerve, the motor branch to the sternocleidomastoid muscle, and the masseteric branch of the trigeminal nerve as alternative inputs for the distal facial trunk. Axonal ingrowth through the distal facial nerve to the target muscles provides resting tone to the facial musculature, and voluntary movement of the tongue, shoulder, or muscle of mastication elicits facial movement. Reinnervation techniques are most commonly employed following skull base tumor resection, when the facial nerve is sacrificed at the brainstem, or when the facial nerve is not actually sacrificed but does not appear to be reaching facial muscle targets after a 12-month waiting period, based upon clinical examination and electrophysiologic studies.
The advantages of the hypoglossal nerve as a donor for reinnervation techniques include its location, close to the extratemporal facial nerve; its dense population of motor axons; and the relative acceptability of the resultant hemitongue weakness. In the classic XII-VII transfer, the entire hypoglossal nerve is transected and reflected superiorly, and a neurorrhaphy to the facial nerve stump is performed (Fig. 178.3A). Several modifications have been described (6) (Fig. 178.3B-D), including the “split” XII-VII transfer, where approximately 30% of the width of the hypoglossal nerve is divided from the main trunk of the nerve for several centimeters, and secured to the lower division of the facial nerve (Fig. 178.3B). Another modification is the XII-VII jump graft, designed to reduce tongue morbidity by avoiding the splicing away of a significant length of the hypoglossal trunk. This involves an end-to-side neurorrhaphy between the hypoglossal nerve and a donor cable graft (usually the great auricular nerve), which in turn is sewn to the distal facial trunk (9) (Fig. 178.3C). This modification evolved from a more precise appreciation of the microanatomy of the hypoglossal nerve, which demonstrates interwoven fascicular architecture; separating a 30% segment away from the main trunk for several centimeters divides a significantly greater number of axons than if the fibers were oriented in parallel.
In circumstances where the facial nerve can be mobilized within the temporal bone and reflected inferiorly, removal of the mastoid tip has permitted direct coaptation of the facial nerve to the hypoglossal nerve, without the need for an interposition graft (see Fig. 178.3D). Elimination of the cable graft provides a theoretical regenerative advantage by reducing from two neurorrhaphies to one.
Surgical Technique
The classic XII-VII procedure is performed via a modified Blair parotidectomy incision. The main trunk of the facial nerve and the pes anserinus are identified using standard facial nerve landmarks. The hypoglossal nerve is identified deep to the posterior belly of the digastric muscle and is followed anteriorly, to just beyond the branching of the descendens hypoglossi. The hypoglossal nerve is sharply transected and reflected superiorly to meet the facial nerve. The facial nerve is transected at the stylomastoid foramen, reflected inferiorly, and secured to the hypoglossal nerve with several 10-0 nylon epineurial microsutures.
The split XII-VII transfer (Fig. 178.3B) provides many fewer axons and is therefore best utilized only for the lower segment of the face. In the jump graft procedure (Fig. 178.3C), the great auricular nerve graft is harvested and interposed between the hypoglossal nerve and the facial stump. For the facial nerve mobilization out of the
temporal bone, the proximal facial nerve is mobilized from the temporal bone via mastoidectomy approach, sectioned at the second genu, and transposed into the neck by removal of the mastoid tip. The facial nerve can be further mobilized by dissecting it away from the parotid tissue beyond its bifurcation. The end-to-side neurorrhaphy is executed by removing a segment of hypoglossal epineurium, then cutting a 30% opening into the hypoglossal nerve and allowing exposure of the severed axons.
temporal bone, the proximal facial nerve is mobilized from the temporal bone via mastoidectomy approach, sectioned at the second genu, and transposed into the neck by removal of the mastoid tip. The facial nerve can be further mobilized by dissecting it away from the parotid tissue beyond its bifurcation. The end-to-side neurorrhaphy is executed by removing a segment of hypoglossal epineurium, then cutting a 30% opening into the hypoglossal nerve and allowing exposure of the severed axons.
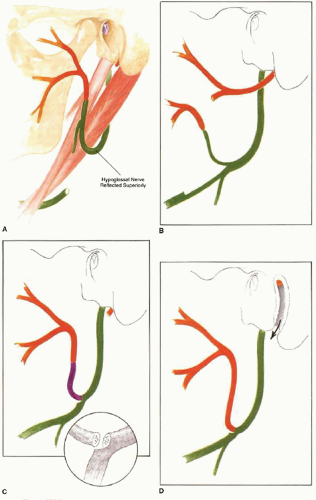 Figure 178.3 Hypoglossal facial nerve transfer. Hypoglossal nerve is shown in green, facial nerve in orange. A: Classic procedure, with entire hypoglossal nerve transected. B: Modification with 40% segment of nerve secured to lower division. C: Jump graft (purple) modification. Insert shows how graft is positioned to capture axons extending from the proximal aspect of the opened hypoglossal nerve. D: Reflection of the facial nerve out of the mastoid bone to meet the hypoglossal nerve in the neck. |
With a XII-VII transfer, good resting facial tone is achieved in over 90% of patients. When successful, the transfer allows deliberate facial movement with intentional manipulation of the tongue. Results are variable, and it is generally agreed that reinnervation must be performed within 2 years following injury, before facial muscle fibrosis and atrophy progress to a point where meaningful tone and movement are not achievable.
Two significant drawbacks of the procedure are the mass facial movement experienced by many patients and the variable tongue dysfunction, which has been categorized as “severe” in up to 25% of patients. Articulation and mastication difficulties are commonly cited. The modifications mentioned above are aimed at one or the other of these two problems. The procedure is contraindicated in patients who are likely to develop other cranial neuropathies (i.e., neurofibromatosis type II) or who have ipsilateral tenth nerve deficits, as the combined X-XII deficit can result in profound swallowing dysfunction.
VII-VII Cross-Face Grafting
Some have advocated utilizing branches of the contralateral facial nerve to drive the denervated facial musculature. It is the only donor source with the potential for mimetic function (the involuntary blink and emotive smile), and it is significantly arborized distally, so several branches may be sacrificed for use in cross-facial grafting, without adversely affecting the healthy side. Donor branches contain many fewer motor axons than the hypoglossal to power the paralyzed side, so the motor input provided by the hypoglossal nerve is distinctly superior. The use of the contralateral facial nerve strictly for reinnervation of native facial musculature has largely been replaced by cross-face nerve grafting in conjunction with free muscle transfer.
ZONAL APPROACH TO THE PARALYZED FACE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


