Facial Reanimation Surgery
Tessa A. Hadlock
Mack L. Cheney
Michael J. McKenna
Facial nerve disorders encompass a broad spectrum of dysfunction, ranging from subtle dynamic facial asymmetry to complete, dense paralysis. Facial nerve regeneration following injury can vary greatly and may result in hypofunction (persistent weakness or poor excursion of facial muscles), hyperfunction (hypertonicity, spasm), or aberrant regeneration (synkinesis). The impact of a facial nerve disorder can be dramatic. Disabilities encountered include corneal exposure of the affected eye, oral incompetence and articulation difficulties from orbicularis oris weakness, and functional nasal obstruction from dilator nares paralysis. None of these is perhaps as significant as the social isolation these patients often succumb to based on their perceived disfigurement and inability to convey emotion through facial expression. Because of the profound effect of this disorder on patient quality of life, a great deal of effort has been focused toward rehabilitation of the paralyzed face.
When facial nerve discontinuity is encountered, the first approach is to attempt to reestablish direct neural continuity between the facial motor nucleus and the distal facial nerve through either primary repair or autografting techniques. When this is not possible, other methods of reestablishing facial balance and movement may be considered. Facial reanimation procedures refer to interventions that restore facial symmetry, resting tone, voluntary movement, or a combination of these. Several broad categories of facial reanimation techniques exist, each appropriate to a specific set of clinical, anatomic, or outcome-related circumstances. These include reinnervation techniques, muscle transfers, and static procedures. The aim of this chapter is to describe each of these approaches, including appropriate clinical scenarios, technical aspects of the surgery, and adjunctive management strategies to optimize postoperative appearance and function.
REINNERVATION TECHNIQUES
Reinnervation techniques, also termed nerve substitution techniques, are procedures that provide neural input to the distal facial nerve and facial musculature via motor nerves other than the native facial nerve. They are indicated in two situations. The first is when the proximal facial nerve stump is not available but the distal facial nerve and facial musculature are present and functional. This occurs following skull base tumor resections involving sacrifice of the nerve at or very close to the brainstem, where neurorrhaphy is not technically achievable. The second situation occurs following skull base surgery, intracranial injury, or traumatic facial paralysis, when the nerve is thought to be anatomically intact but there is no discernable return of function after a satisfactory waiting period of 12 months. Lack of functional recovery, electrophysiologic demonstration of lack of reinnervation potentials, and the presence of fibrillation potentials at 12 months indicate persistent complete denervation. This suggests insufficient regenerative potential from the proximal facial nerve stump and therefore mandates alternative proximal axonal input to the distal facial nerve and facial musculature.
Hypoglossal-Facial Transfer (XII-VII Crossover)
The nerve most often utilized to reinnervate the distal facial nerve is the hypoglossal nerve. Its proximity to the extratemporal facial nerve, its dense population of myelinated motor axons, the relative acceptability of the resultant hemitongue weakness, and the highly predictable and reliable result make it a logical choice (1, 2, 3, 4). In the classic XII-VII transfer, the entire hypoglossal nerve is transected and reflected upward for direct neurorrhaphy to the facial nerve stump (Fig. 38.1A). Several modifications have been described (Fig. 38.1B, C-D), including the “split” XII-VII transfer (5), in which approximately 30% of the width of the hypoglossal nerve is divided from the main trunk of the nerve for several centimeters and secured to the lower division of the facial nerve (Fig. 38.1B). Another modification, designed to reduce tongue morbidity by avoiding the splicing away of a significant length of the partial hypoglossal trunk, is the XII-VII jump graft. This involves an end-to-side neurorrhaphy between the hypoglossal nerve and a donor cable graft (usually the great auricular nerve), which in turn is sewn to the
distal facial trunk (6) (Fig. 38.1C). This modification is based upon improved appreciation of the microanatomy of the hypoglossal nerve, which demonstrates interwoven fascicular architecture; separating a 30% segment away from the main trunk for several centimeters divides a significantly greater number of axons than if the fibers were oriented in parallel (6).
distal facial trunk (6) (Fig. 38.1C). This modification is based upon improved appreciation of the microanatomy of the hypoglossal nerve, which demonstrates interwoven fascicular architecture; separating a 30% segment away from the main trunk for several centimeters divides a significantly greater number of axons than if the fibers were oriented in parallel (6).
In some circumstances where the facial nerve is able to be mobilized from the second genu within the temporal bone and reflected inferiorly, removal of the mastoid tip allows for direct coaptation of the facial nerve to the hypoglossal without the need for an interposition graft (7) (Fig. 38.1D). Elimination of the cable graft provides a theoretical regenerative advantage by reducing from two neurorrhaphies to one.
Surgical Technique
The classic XII-VII procedure is performed via a modified Blair parotidectomy incision. The main trunk of the facial nerve and the pes anserinus are identified using standard facial nerve landmarks, such as the tragal pointer and the tympanomastoid suture line. The hypoglossal nerve is then located in its ascending portion, deep to the posterior belly of the digastric, along the medial surface of the internal jugular vein. The nerve is followed anteriorly and freed of fascial attachments beyond the takeoff of the descendens hypoglossi. The hypoglossal nerve is then sharply transected and reflected superiorly to meet the facial nerve. The facial nerve is transected at the stylomastoid foramen, and the entire distal trunk is reflected inferiorly and secured to the hypoglossal nerve with 5 to 7 10-0 nylon epineurial microsutures.
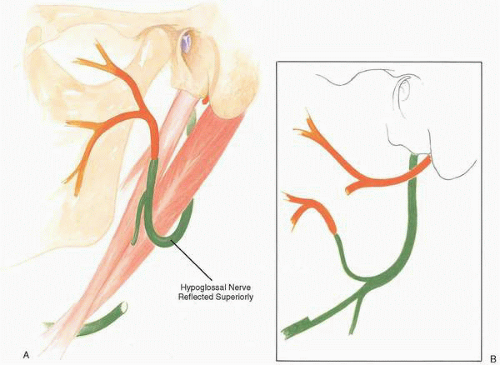 FIG. 38.1 Hypoglossal facial nerve transfer. Hypoglossal nerve is shown in green, facial nerve in orange. A: Classic procedure, with entire hypoglossal nerve transected. B: Modification with 40% segment of nerve secured to lower division. Hypoglossal facial nerve transfer. Hypoglossal nerve is shown in green, facial nerve in orange. C: Jump graft (purple) modification. Insert shows how graft is positioned to capture axons extending from the proximal aspect of the opened hypoglossal nerve. D: Reflection of the facial nerve out of the mastoid bone to meet the hypoglossal nerve in the neck. |
A modification designed to decrease mass movement of the face involves sectioning the entire facial nerve but performing a neurorrhaphy only to the inferior division of the facial nerve, or ligating the upper division distal to the pes (Fig. 38.1), and employing separate techniques for management of the upper face. The split XII-VII transfer provides many fewer axons and is therefore best utilized only for the lower segment of the face.
In the jump graft or direct XII-VII end-to-side procedure, once the exposure has been obtained the great auricular nerve graft is harvested or the proximal facial nerve is mobilized from the temporal bone, sectioned at the second genu,
and transposed into the neck by removal of the mastoid tip. The facial nerve can be further mobilized by dissecting it away from the parotid tissue beyond its bifurcation. The end-to-side neurorrhaphy is executed by removing a segment of hypoglossal epineurium, then cutting a 30% opening into the hypoglossal nerve and allowing the defect to open up. The recipient nerve is then laid into the defect, facing the proximal cut surface, and secured with microsutures.
and transposed into the neck by removal of the mastoid tip. The facial nerve can be further mobilized by dissecting it away from the parotid tissue beyond its bifurcation. The end-to-side neurorrhaphy is executed by removing a segment of hypoglossal epineurium, then cutting a 30% opening into the hypoglossal nerve and allowing the defect to open up. The recipient nerve is then laid into the defect, facing the proximal cut surface, and secured with microsutures.
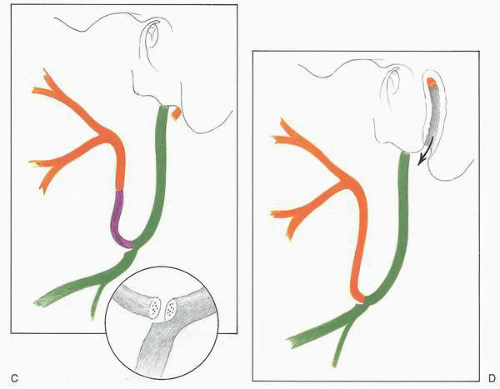 FIG. 38.1, cont’d. |
Results, Drawbacks, and Contraindications
With a XII-VII transfer, good resting facial tone is achieved in more than 90% of patients. When successful, the transfer allows deliberate facial movement with intentional manipulation of the tongue. Recovery generally occurs over 6 to 24 months and in some cases has been reported to continue up to 5 years. Results are variable, with time from denervation to transfer playing a key role in outcome. There is general consensus that reinnervation must occur within 2 years following injury, otherwise neuromuscular fibrosis and atrophy progress to a point where meaningful tone and movement are not achievable (6).
The two most significant drawbacks of the procedure are the mass facial movement experienced by many patients and the variable tongue dysfunction, which has been categorized as severe in up to 25% of patients. Articulation and mastication difficulties are commonly cited. The modifications mentioned earlier are aimed at one or the other of these two problems. In addition, botulinum toxin administration in the region of the eye and physical therapy have proven useful adjuncts for patients with clinically significant mass movement.
The procedure is contraindicated in patients who are likely to develop other cranial neuropathies (e.g., neurofibromatosis type II) or who have ipsilateral tenth nerve deficits, as the combined X-XII deficit can lead to profound swallowing dysfunction.
VII-VII CROSS FACIAL GRAFTING
Another potential source of axons for facial reinnervation is the contralateral healthy facial nerve (8). The two distinct advantages of its use are that it is the only donor source with the potential for mimetic function (the involuntary blink and
emotive smile) and that it is significantly arborized distally, so several branches may be sacrificed for use in cross facial grafting, usually without adversely affecting the healthy side. The disadvantages include many fewer motor axons than the hypoglossal, with unpredictable results; the need for a lengthy sural nerve jump graft; and the potential for facial weakness on the donor side (9). Most surgeons feel the motor power provided by the hypoglossal nerve is distinctly superior, and the use of the contralateral facial nerve strictly for reinnervation of native facial musculature has largely been replaced by cross face nerve grafting in conjunction with free muscle transfer.
emotive smile) and that it is significantly arborized distally, so several branches may be sacrificed for use in cross facial grafting, usually without adversely affecting the healthy side. The disadvantages include many fewer motor axons than the hypoglossal, with unpredictable results; the need for a lengthy sural nerve jump graft; and the potential for facial weakness on the donor side (9). Most surgeons feel the motor power provided by the hypoglossal nerve is distinctly superior, and the use of the contralateral facial nerve strictly for reinnervation of native facial musculature has largely been replaced by cross face nerve grafting in conjunction with free muscle transfer.
Surgical Technique
The VII-VII cross facial graft technique has a great deal of surgical variability with regard to exposure of the donor and recipient nerves, the length and positioning of jump grafts, and the timing of second stage neurorrhaphy. There are insufficient data to allow specific approaches to emerge as superior to others (10, 11, 12). It is ordinarily a staged procedure, where in the first stage a sural nerve graft is harvested from the leg, tunneled subcutaneously from the ipsilateral preauricular region across the face, and sewn to the fresh-cut edges of one or several buccal branches of the functioning facial nerve (Fig. 38.2), via a nasolabial fold or a preauricular incision. The growth of axons into the graft is followed clinically by tapping on the graft (Tinel’s sign); tingling indicates the presence of regenerating axons. Once regeneration has occurred across the face, a second stage is performed where the sural nerve graft is sewn to one or several branches of the affected facial nerve. Alternatively, the ipsilateral neurorrhaphy can be performed in the same operative setting.
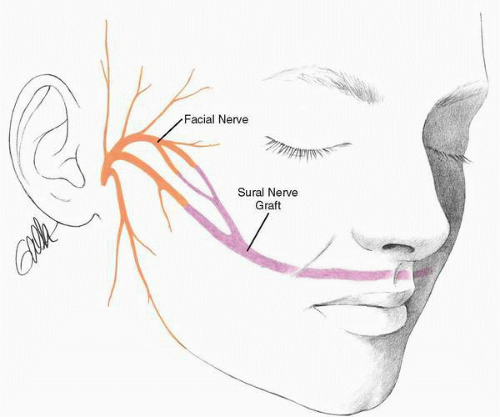 FIG. 38.2 Placement of a cross face nerve graft. Note that several midface branches are sacrificed and routed into the graft. |
Results, Drawbacks, and Contraindications
The major disadvantage with cross facial nerve grafting is that results are inconsistent. Some authors report excellent recovery, whereas many others find it entirely unsatisfactory. It appears that it is most useful in association with other reanimation modalities, to address a single territory within the face rather than to reinnervate the entire contralateral facial nerve. Recent studies employing the cross facial graft for isolated marginal mandibular paralysis demonstrate its utility (13).
OTHER REINNERVATION TECHNIQUES
Several other cranial nerves have been employed for reinnervation of the distal facial nerve stump. The spinal accessory nerve (14), glossopharyngeal nerve, and trigeminal nerve have all been described as potential donors, though none has gained great popularity. The donor morbidity and difficulty with surgical exposure far exceed that found with XII-VII and cross facial grafting. Experimentation with utilizing
isolated branches, such as the sternocleidomastoid branch of the spinal accessory nerve (15,16), would decrease donor morbidity, potentially increasing the utility of this technique.
isolated branches, such as the sternocleidomastoid branch of the spinal accessory nerve (15,16), would decrease donor morbidity, potentially increasing the utility of this technique.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


