Emotions are communicated through facial expression. Happiness, confusion, and frustration can be expressed with a slight smile, eyebrow shift, or wrinkled nose. Injury to the facial nerve and subsequent inability of perform volitional mimetic movement can provoke anxiety. This article explores the causes, treatment, and prevention of facial nerve paralysis.
Emotions are communicated through facial expression. Happiness, confusion, and frustration can be expressed with a slight smile, eyebrow shift, or wrinkled nose. Injury to the facial nerve and subsequent inability of perform volitional mimetic movement can provoke anxiety . This article explores the causes, treatment, and prevention of facial nerve paralysis.
Overview
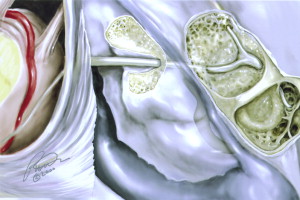
The facial nerve traverses a bony canal in the temporal bone as it courses from the brainstem to the face and neck. The narrowest portion of this canal is the meatal segment, which is located at the transition zone between the lateral portion of the internal auditory canal and the proximal fallopian canal ( Fig. 1 ). Depending on the extent of injury sustained, the facial nerve will lose function in a graduated fashion. If edema is minimal, the nerve will be anatomically intact and a conduction blockade (neuropraxia) will be the only result, and the nerve will recover function quickly and fully without deficit. As nerve injury increases so do sequela from the injury . As the edema increases, the nutrients to the nerve diminish as axoplasmic flow decreases. This decrease in flow ultimately results in axonal death (axonotmesis) . The axon will degenerate in a retrograde fashion to the narrowest portion of the facial canal. With this type of injury, the endoneurium is intact and the axon will regrow through the undisturbed axonal channels, resulting in normal facial function. Any increased injury at this point will result in disruption of the endoneurium (neurotmesis), allowing the regenerating axons to regrow haphazardly. Depending on the extent of nerve disruption this haphazard growth will lead to a variable degree of synkinesis .
As a general rule, all patients who have facial paralysis should undergo imaging studies to evaluate the course of the nerve from the brain through the parotid. This evaluation is best performed with a thin-cut contrasted MRI through the temporal bone and upper neck. Patients who have facial paralysis secondary to trauma should undergo a thin-cut temporal bone CT scan .
Bell’s palsy
Rapidly progressive facial paralysis over 24 or 48 hours is most likely secondary to idiopathic nerve edema. The nerve edema is believed to be caused by a viral insult from either activation of a latent herpetic infection or a newly acquired upper respiratory track virus. Bell’s palsy is differentiated from other causes of facial paralysis by the absence of trauma and its rapid onset over several hours. This history of rapid progression helps differentiate it from facial paralysis secondary to tumor involvement, which progresses slowly over weeks to months.
Facial paralysis secondary to viral insult is usually self-limited. Depending on the extent of the nerve edema, recovery occurs within days to weeks but can take several months in severe cases. Initiating steroids early (prednisone, 1 mg/kg, for 1 week with a taper) can minimize progressive edema, diminishing further nerve damage and speeding recovery. Studies have shown mixed results on the efficacy of empiric use of antiviral medication. However, valacyclovir was recently associated with earlier recovery and better long-term facial nerve function .
Patients who have observable facial movement with an incomplete paralysis experience uniformly good recovery. Recovery may be prolonged and incomplete for patients who have a dense House-Brackmann 6 paralysis ( Table 1 ). Some authors advocate decompressing the facial nerve if facial nerve degeneration is rapid and severe . Although literature supports facial nerve decompression for severe cases of Bell’s palsy, the recovery rate remains good without surgical intervention and most surgeons reserve decompression for patients who have recurrent paralysis.
| Class | General | Symmetry at rest | Synkinesis | Movement | Eye closure |
|---|---|---|---|---|---|
| 1 | Normal | Yes | No | Normal | Yes |
| 2 | Slight Weakness | Yes | No | Weak | Yes |
| 3 | Can close eye | Yes | Yes | Weak | Yes |
| 4 | Cannot close eye | Yes | Yes | Weak | No |
| 5 | Slight movement | No | Yes | Slight | No |
| 6 | Paralyzed | No | N/A | No | No |
Bell’s palsy
Rapidly progressive facial paralysis over 24 or 48 hours is most likely secondary to idiopathic nerve edema. The nerve edema is believed to be caused by a viral insult from either activation of a latent herpetic infection or a newly acquired upper respiratory track virus. Bell’s palsy is differentiated from other causes of facial paralysis by the absence of trauma and its rapid onset over several hours. This history of rapid progression helps differentiate it from facial paralysis secondary to tumor involvement, which progresses slowly over weeks to months.
Facial paralysis secondary to viral insult is usually self-limited. Depending on the extent of the nerve edema, recovery occurs within days to weeks but can take several months in severe cases. Initiating steroids early (prednisone, 1 mg/kg, for 1 week with a taper) can minimize progressive edema, diminishing further nerve damage and speeding recovery. Studies have shown mixed results on the efficacy of empiric use of antiviral medication. However, valacyclovir was recently associated with earlier recovery and better long-term facial nerve function .
Patients who have observable facial movement with an incomplete paralysis experience uniformly good recovery. Recovery may be prolonged and incomplete for patients who have a dense House-Brackmann 6 paralysis ( Table 1 ). Some authors advocate decompressing the facial nerve if facial nerve degeneration is rapid and severe . Although literature supports facial nerve decompression for severe cases of Bell’s palsy, the recovery rate remains good without surgical intervention and most surgeons reserve decompression for patients who have recurrent paralysis.
| Class | General | Symmetry at rest | Synkinesis | Movement | Eye closure |
|---|---|---|---|---|---|
| 1 | Normal | Yes | No | Normal | Yes |
| 2 | Slight Weakness | Yes | No | Weak | Yes |
| 3 | Can close eye | Yes | Yes | Weak | Yes |
| 4 | Cannot close eye | Yes | Yes | Weak | No |
| 5 | Slight movement | No | Yes | Slight | No |
| 6 | Paralyzed | No | N/A | No | No |
Iatrogenic
Iatrogenic trauma to the facial nerve should be addressed as soon as the injury is recognized. Optimal choices for reconstruction depend on the site of injury and the length of nerve involved.
Unintentional iatrogenic facial nerve paralysis is traumatic for patients and physicians. Operating surgeons often should obtain a second opinion from an experienced physician who can offer an unemotional objective assessment of the severity of injury and propose appropriate treatment options .
Fortunately, one of the more common causes of unintentional iatrogenic facial nerve paralysis is overzealous use of local anesthetic. In an attempt to obtain adequate anesthesia, particularly for surgical cases performed primarily using local anesthesia, physicians may be tempted to use more anesthetic than they would otherwise. The anesthetic may track along the stylomastoid suture line and anesthetize the facial nerve at the stylomastoid foramen. When facial nerve injury is not expected and a patient experiences immediate postoperative paralysis, physicians may want to wait a few hours to allow the effects of the local anesthetic to wear off before deciding whether further intervention is needed. Frequently, facial function will begin returning within an hour if lidocaine was used, or longer if Marcaine was used. Once adequate time is allowed for the effects of local anesthesia to dissipate and the patient continues to show complete facial paralysis, the facial nerve should be identified and its course followed to locate the site of injury .
For patients who have undergone otologic surgery, the facial nerve should be identified at the proximal tympanic segment as it courses from the geniculate ganglion superior to the cochleariform process, and followed to the pyramidal turn down to the stylomastoid foramen ( Fig. 2 ). All areas along the course of the intratemporal facial nerve are potential sites of injury. When dissecting cholesteatoma in the epitympanum and supratubal recess, the geniculate ganglion and proximal tympanic segment of the facial nerve are at risk for injury . The cochleariform process, which is the exit site of the tensor tympani tendon, is an excellent landmark for the tympanic portion of the facial nerve as it passes just superior to it. The pyramidal turn is another vulnerable site as the nerve turns from its course under the horizontal semicircular canal and descends through the mastoid to the stylomastoid foramen . A blood vessel supplying the nerve in this area is often present to warn the surgeon that the nerve is near by .
The descending or mastoid portion of the nerve can also be injured. A common practice for identifying the facial nerve is to open the mastoid air cells, identify the horizontal semicircular canal, and follow the digastric ridge to the stylomastoid foramen and then thin the external auditory canal in a stepwise fashion, working lateral to medial between the landmarks of the stylomastoid foramen and the horizontal semicircular canal. The descending portion of the facial nerve tracks laterally as it progresses to the stylomastoid foramen and may be lateral to the tympanic ring inferiorly . This important anatomic relationship is important when performing a canaloplasty. The facial nerve is vulnerable to injury when expanding the canal in a posterior inferior direction (see Fig. 2 ).
Once the site of nerve injury is identified, if disruption to the nerve is 50% or less than the total cross-sectional area, then adequate function should return and it is best to leave the nerve alone to minimize any further damage. If more than 50% is traumatized, then the injured portion of the nerve should be removed and an end-to-end anastomosis performed . It is important that a tension-free anastomosis is performed. Tension increases the amount of fibrotic in growth and subsequently decreases the number of axons that are able to propagate distally. If extra nerve length is needed, then the fallopian canal should be opened from the cochleariform process to the stylomastoid foramen. The nerve can then be rerouted directly from these two landmarks, thereby straightening the pyramidal turn and gaining approximately 1 cm in length to perform a tension-free end-to-end anastomosis .
If the length of nerve damage is greater than can be compensated for by rerouting, a nerve graft should be used. Many potential sites are available to harvest nerve for a cable graft, but the most commonly used are the great auricular nerve and the sural nerve.
Temporal bone fracture
Fractures of the temporal bone are typically comminuted and vary tremendously depending on the mechanism of injury. Despite the variability that occurs with temporal bone fractures, they can generally be categorized into two groups based on the location of the major fracture lines and how they relate to the axis of the petrous pyramid. When the fracture line is parallel to the posterior petrous face, it is categorized as a longitudinal fracture; when it runs perpendicular across the posterior petrous face, it is a transverse fracture. Most significant facial nerve injury, caused by nonpenetrating temporal bone trauma, occur in the perigeniculate area as a consequence of traction injury from the greater superficial petrosal nerve (GSPN) ( Fig. 3 ) .



