Although often listed together in review articles and case series, tracheobronchial and esophageal foreign bodies can be dissimilar. Airway foreign bodies can range widely in the severity of presentation. When to proceed with a diagnostic bronchoscopy is not always obvious and is based on three diagnostic tools: clinical history, physical examination, and radiography. Radiography plays a more central role in the diagnosis of an esophageal foreign body. In either condition, a delay in diagnosis leads to a greater complication rate. This article provides diagnostic and treatment guidelines in the management of aerodigestive foreign bodies.
Airway foreign bodies
Airway foreign bodies (AFBs) have remained a diagnostic challenge to health care professionals. They can become life-threatening emergencies that require immediate intervention or can go unnoticed for weeks and even months. Every effort must be made to avoid a delay in diagnosis because this may lead to a notable increase in complication rates . A sudden onset of respiratory symptoms must alert the clinician to the presence of an AFB. This section presents an overview of the assessment and management of patients who have potential AFBs.
Initial patient assessment
Clinical presentation
AFBs most commonly occur in the 1- to 3-year-old child and may be related to immature dentition and a poorly coordinated swallowing mechanism. In addition, children in this age group are more likely to be active while eating and are prone to introducing various objects into their mouth. When the aspiration of a foreign body is witnessed by the caregiver, the following characteristic symptoms are often described: an early choking or gagging episode, followed by a coughing spell. As the foreign body moves distally in the airway, the symptoms often become less apparent and may even subside, creating a great diagnostic challenge because the remainder of the assessment, mainly the physical examination and radiography, can be deceptively normal . Therefore, the incipient event that leads the caregiver to bring the child to a health care professional can be the most important factor in the decision to proceed with a diagnostic airway endoscopy.
The classic triad of sudden onset of paroxysmal coughing, wheezing, and diminished breath sounds on the ipsilateral side is not present in all cases of foreign body aspiration. Linegar and colleagues reported that among children who had a positive clinical history and a negative chest radiograph and physical examination, there was a 45% incidence of foreign bodies on airway endoscopy. They also found that in children who had a “doubtful” history, the positive yield on endoscopy was only 9.5%. Ciftci and colleagues reported that a positive history was the most sensitive (91%), accurate (84%), and specific (46%) of all the diagnostic tools. Table 1 illustrates a wide range in the reported sensitivities and specificities among the three main diagnostic tools.
| Study [Ref.] | N | History | Physical examination | Radiography | |||
|---|---|---|---|---|---|---|---|
| Sensitivity (%) | Specificity (%) | Sensitivity (%) | Specificity (%) | Sensitivity (%) | Specificity (%) | ||
| Ciftci et al, 2003 | 663 | 91 | 46 | 86 | 26 | 88 | 30 |
| Zerella et al, 1998 a | 293 | 86 | 82 | 24 | 64 | 49 | n/a |
| Hoeve et al, 1993 | 115 | 81 | 33 | 78 | 37 | 82 | 44 |
| Barrios et al, 1997 | 100 | 97 | 63 | n/a | n/a | 85 | 9 |
| Metrangelo et al, 1999 | 87 | 96 | 76 | 84 | 12 | 70 | 63 |
| Evan et al, 2005 | 98 | 91 | 45 | 80 | 60 | 68 | 71 |
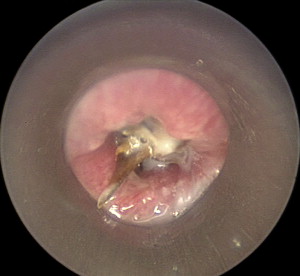
Peanuts, seeds, and beans are the most common aspirated matter. Peanuts and other organic objects may cause significant tissue reaction, leading to the development of granulation tissue ( Fig. 1 ). The shape and consistency of the aspirated item can also affect the clinical picture. Relatively narrow and oval objects (such as lima beans) can change position in the airway and lead to intermittent complete airway obstruction. Grains, beans, and other vegetable matter may absorb water and can have a more rapid clinical deterioration ( Fig. 2 ).

Physical examination
The presentation of an individual who has an AFB can range from a patient who is quiet and without discomfort to one who may exhibit signs of severe distress and impending respiratory failure. In general, the physical examination tends to have a low specificity and a variable yet higher sensitivity in predicting AFBs (see Table 1 ). Careful auscultation of the chest is the most critical part of the physical examination. Findings include unilateral wheezing and a discrepancy in breath sounds. Because many investigators have reported a relatively high incidence of normal physical findings (14%–45%) in patients diagnosed with an AFB on bronchoscopy , a negative physical examination should not be used to rule out the presence of an AFB. Its relatively high sensitivity, however, suggests that a positive physical examination can be a very useful tool in establishing a need for bronchoscopy.
Radiography
Plain radiographs can play an important role in the evaluation of a patient suspected of having an AFB. Although most AFBs tend to be radiolucent (∼80%), certain radiograph findings can be useful in reaching a diagnosis. As the cross-sectional area of the airway increases during inspiration, air can pass beyond the foreign body. During expiration, as the cross-sectional area decreases, the air can become “trapped.” Films taken during expiration can reveal hyperinflation at the ipsilateral lung ( Fig. 3 ). This phenomenon may be less common than previously presumed .

Atelectasis can be seen when the aspirated object completely obstructs the distal airway. Atelectasis and pneumonia are findings more commonly seen in the setting of delayed diagnosis (after 24 hours). Airway fluoroscopy, where available, can be a useful asset to the experienced radiologist but may have a lower sensitivity and specificity than chest radiography .
The clinician must always consider the limitations of radiography in the diagnosis of AFBs. Radiographs should not be used to rule out the presence of an AFB but used to aid in its diagnosis. Over one half of tracheal foreign bodies and 25% of bronchial foreign bodies have normal plain chest radiographs . The reported diagnostic sensitivity (49%–88%) and specificity (9%–71%) of radiographs is inconsistent and may suggest that the true yield of radiography may rely a great deal on the availability of experienced radiologists (see Table 1 ). Compared with history and physical examination, radiography appears to be the least sensitive in predicting bronchoscopy findings .
It is important to emphasize that a patient who presents with a classic history for an AFB and who may have an unpredictable or unstable airway should not be sent to a relatively unmonitored location for a radiograph. This protocol is especially relevant in younger children because the potential agitation from a chest radiograph may lead to sudden airway compromise. The use of radiography should be limited to patients who are deemed to have a stable airway and when the decision to proceed with endoscopy is in question.
Treatment recommendations
Indications for endoscopy
A delay in diagnosis is likely to increase the risk of intraoperative and postoperative complications . To prevent a diagnostic delay, a witnessed choking event followed by a period of coughing should be considered an acceptable indication for bronchoscopy, without relying on other diagnostic tools . The diagnostic tools used in the assessment of an AFB have been shown to have relatively high sensitivities, with poor and variable specificities (see Table 1 ). A good rule of thumb is that diagnostic bronchoscopy should be performed if any one of the three diagnostic tools (history, physical examination, or radiography) is considered positive. Furthermore, if any one of these is negative, the possibility of an AFB remains.
Many cases do not present with straightforward positive or negative findings. When the findings on physical examination, radiographs, or both are questionable, there is good evidence suggesting that both tools increase their diagnostic yield 24 hours after the event of aspiration . For this reason, when the diagnosis is in question in a stable patient, the clinician can consider repeating radiography and the physical examination after a 24-hour period.
Preoperative care and anesthesia
After the diagnosis of an AFB is entertained, a patient should remain calm and monitored. The duration of fasting before endoscopy should be based on the clinician’s assessment of airway stability. In acute cases of aspiration when the patient is considered unstable or potentially unstable, securing the airway should take precedence over fasting guidelines. Tomaske and colleagues found that among 31 children who had symptoms of acute airway obstruction and underwent bronchoscopy without long fasting periods (<2 hours), no cases of pulmonary aspiration from gastric contents were seen. When the child is considered stable, however, the timing of endoscopy should be based on preoperative fasting guidelines and the availability of skilled personnel.
Endoscopy and foreign body removal
Extraction of the AFB requires significant skill to avoid incurring further trauma to the respiratory epithelium. The surgeon must carefully avoid pushing the foreign body distally and making the retrieval more challenging.
The skill of the anesthesiologist is also of critical importance during this procedure. It is preferable to keep the patient breathing spontaneously because this avoids significant amounts of positive pressure ventilation that may induce distal migration of the foreign body. Furthermore, during natural inspiration, the tracheal/bronchial cross-sectional area increases and may allow better access to tightly lodged foreign bodies. For spontaneous ventilation to be successful, it is imperative that the surgeon adequately anesthetize the glottis and distal airway (especially the carina) before attempting foreign body retrieval. The author’s preference is to use 2% lidocaine sprayed topically to the glottis, trachea, and carina. This methodology assists the anesthesiologist in maintaining the patient’s spontaneous breathing without sudden movements that can seriously complicate the procedure.
Age-appropriate equipment is crucial for preventing further trauma to the respiratory epithelium. The surgeon’s familiarity with a wide assortment of laryngoscopes, bronchoscopes, and optical forceps facilitates the retrieval process and prevents unnecessary intraoperative delays. There must always be two bronchoscopes available; one that is age appropriate and one that is one size smaller.
Often the object is too large to pass through the lumen of the bronchoscope and must be removed as a single unit along with the bronchoscope and the optical forceps. When the object is sharp and facing the proximal airway, it is more safely removed when it is enclosed within the lumen of the bronchoscope .
Postoperative care
Chest physiotherapy can be useful in the postoperative period to help mobilize secretions and to prevent an infection. Antibiotics are not routinely used in acute cases but can play an important role in cases of delayed diagnosis (see later discussion). Generally, in the absence of complications, there are no notable interventions necessary in the postoperative setting.
Complications
Delay in diagnosis presents a significant increase in perioperative morbidity . Total or near-total mainstem bronchial obstruction leads to poor alveolar aeration and subsequent shunting of pulmonary perfusion away from the affected lung. When the foreign body migrates to the contralateral side, the patient can experience abrupt respiratory decompensation . This scenario is intensified in cases of delayed diagnosis because the body has more time to compensate for unilateral decrease in ventilation. Delayed diagnosis is further complicated by the development of pneumonia, atelectasis, and granulation tissue, which can lead to significant bleeding on removal of the foreign body (see Fig. 3 ).
Complications from bronchoscopy can also include postoperative stridor , bronchospasm, hypoxia, transient arrhythmias, and bradycardia. In a large case series of 3300 patients, the mortality rate was reported to be a little less than 1% .
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


