28
Facial Nerve Disorders
Pamela C. Roehm, Jay T. Rubenstein, and Bruce J. Gantz
Proper management of facial nerve disorders requires an appreciation for the wealth of knowledge about this cranial nerve and for the gaps in our understanding of its pathophysiology. Many facial nerve disorders are extremely rare and their natural history is poorly documented. Other disorders, such as Bell’s palsy, are common and the natural history well known. Unfortunately, this knowledge does little to decrease the controversy regarding appropriate management of the disease. It is unlikely that there will be a consensus regarding management of all the disorders described in this chapter. However, when a patient presents with a disorder of the facial nerve, the clinician must advise and provide treatment. In many cases it is appropriate to offer more than one treatment plan and allow the patient to choose, based on the known risks and benefits of that plan. In these situations the patient must be aware of the unknowns inherent in any approach.
 Anatomy of the Facial Nerve
Anatomy of the Facial Nerve
The facial nerve has a complex three-dimensional course from its motor nucleus in the anterior pons to its insertion into the muscles of facial expression. After exiting posteriorly from the motor nucleus, fibers of the facial nerve turn abruptly around the abducens nucleus and exit from the brainstem at the pontomedullary junction. At its exit from the brainstem, the facial nerve lies 1.5 mm anterior to the eighth cranial nerve. The nervus intermedius, which is composed of parasympathetic fibers that become the greater superficial petrosal and chorda tympani nerves, exits the brainstem between cranial nerves VII and VIII. The facial nerve is about 1.8 mm in diameter at its root entry zone. After leaving the brainstem, it has a 15- to 17-mm course through the cerebellopontine angle (CPA) prior to entering the porus of the internal auditory canal (IAC). Within the CPA the facial nerve is in close proximity to the anterior inferior cerebellar artery (AICA), which provides the vascular supply to this segment of the nerve. The AICA may lie anterior to or between cranial nerves VII and VIII. Occasionally, a loop of AICA may course laterally to the fundus of the IAC.
After entering the IAC, the facial nerve travels 8 to 10 mm prior to entering the meatal foramen (Fig. 28–1). In the IAC it occupies the anterior-superior quadrant and at the fundus it is separated from the superior vestibular nerve by the vertical crest (Bill’s bar) and from the cochlear nerve by the transverse crest. On entering the meatal foramen, the facial nerve narrows to its smallest diameter, 0.61 to 0.68 mm. The ratio of the fallopian canal diameter to facial nerve diameter is at its lowest as well. Adour1 has questioned the concept of meatal entrapment as a mechanism for facial nerve injury, but there are now substantial data demonstrating that entrapment at the meatal foramen and labyrinthine segment plays a role in the pathogenesis of at least some facial nerve disorders as detailed below.2–13
The labyrinthine segment is 4 mm in length between the meatal foramen and the geniculate ganglion. It is located immediately posterior and slightly superior to the basal turn of the cochlea. The labyrinthine segment is just anterior to the ampulla of the superior semicircular canal and courses superiorly as it travels laterally, a position of importance for middle fossa surgery. At the geniculate ganglion, the nerve takes a 75-degree turn posteriorly into the tympanic segment. The greater superficial petrosal nerve (GSPN) exits the fallopian canal via the facial hiatus with the superficial petrosal artery (a branch of the middle meningeal artery), which is the vascular supply to this region of the nerve.
The tympanic segment is about 11 mm long and lies between the takeoff of the GSPN and the second genu. It forms the superior aspect of the oval window niche and is readily injured by pathologic processes and unwary middle ear surgeons, due to its frequently occurring dehiscences.14,15
After passing between the stapes and the lateral semicircular canal, the nerve turns inferiorly into the mastoid segment. This measures 13 mm in length down to the stylomastoid foramen. The stylomastoid artery, a branch of the postauricular artery, supplies this portion of the nerve. Dense connective tissue envelops the nerve as it exits the stylomastoid foramen. During procedures that require mobilization of this portion of the facial nerve, nerve injury can be avoided by including a margin of the connective tissue with the nerve during mobilization.16
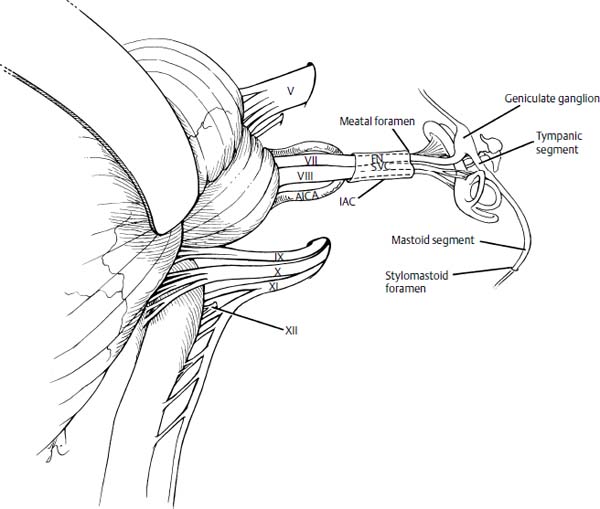
Figure 28–1 Course and relationships of the left facial nerve from the pontomedullary junction to the stylomastoid foramen. AICA, anterior inferior cerebellar artery; IAC, internal auditory canal; FN, facial nerve; SVN, superior vestibular nerve.
 Grading of Facial Weakness
Grading of Facial Weakness
Assessment of treatment efficacy requires a consistent system for grading facial weakness. The House-Brackmann scale17 was originally developed for assessment of outcome in Bell’s palsy but has proven useful in management of all acute facial nerve disorders. It is listed in Table 28–1.
 Facial Nerve Disorders in Adults
Facial Nerve Disorders in Adults
Bell’s Palsy
One should expect that any fairly common disorder with a well-described natural history, multiple placebo-controlled treatment trials, a wealth of intraoperative observation, and morphologic, histopathologic, electrophysiologic, and molecular data would be treatable with a minimum of controversy. This is far from true in the case of the acute facial paralysis first described by Sir Charles Bell. The debate over the efficacy of any medical or surgical therapy has changed its focus over time, but the fundamental disagreements have not changed in 30 years. Nevertheless, much is known about the natural history, possible etiologies, pathogenesis, and clinical evaluation of the patient with Bell’s palsy, so that a treatment algorithm may be formed and allows for unknown and debatable issues. An excellent review of these issues is available.18
Diagnosis
Although Bell’s palsy may not be idiopathic,1 it remains a diagnosis of exclusion. The clinician must exclude all identifiable causes of facial paralysis that may be determined by history, physical examination, or radiologic study. It is not uncommon for CPA tumors, skull base neoplasms, otitis media, or parotid lesions to be misdiagnosed as Bell’s palsy. These errors should be rare, as history and physical examination point to the correct diagnosis the vast majority of the time. A partial or total unilateral facial paralysis with onset over a 48-hour period without hearing loss, vertigo, or other cranial neuropathy and with a normal head and neck examination is likely to be Bell’s palsy. Other than audiometric evaluation, it does not require further diagnostic workup except for HIV testing or Lyme titers in appropriate circumstances. Some recovery should be noted within 3 to 6 months in all patients.
Occasionally, a sudden total facial paralysis occurs that does not resolve in 6 months. This situation requires thorough imaging and possibly surgical exploration prior to any attempt at reanimation. Parotid malignancy has been reported as long as 10 years after acute facial palsy.19 A case of fluctuating facial paralysis has been seen in our institution in association with negative enhanced magnetic resonance imaging (MRI) and high-resolution temporal bone computed tomography (CT). An occult parotid malignancy was diagnosed 6 months later. Another case of acute facial paralysis 6 months after excision of a squamous cell carcinoma of the cheek skin proved to be metastatic carcinoma despite multiple negative imaging studies. These cases are unusual but point to the necessity of aggressive evaluation of all progressive facial pareses, segmental pareses, pareses associated with facial twitching prior to onset, pareses associated with other cranial neuropathies, and those acute palsies that do not show some recovery within 6 months.
| Grade | Description | Characteristics | ||
|---|---|---|---|---|
| I | Normal | Normal facial function in all areas | ||
| II | Mild dysfunction | Gross: slight weakness noticeable on close inspection; may have very slight synkinesis | ||
| At rest: normal symmetry and tone | ||||
| Motion | ||||
| Forehead: moderate to good | ||||
| Eye: complete closure with minimum effort | ||||
| Mouth: slight asymmetry | ||||
| III | Moderate dysfunction | Gross: obvious but not disfiguring difference between two sides; noticeable but not severe synkinesis, contracture, and/or hemifacial spasm | ||
| At rest: normal symmetry and tone | ||||
| Motion | ||||
| Forehead: slight to moderate movement | ||||
| Eye: complete closure with effort | ||||
| Mouth: slightly weak with maximum effort | ||||
| IV | Moderately severe dysfunction | Gross: obvious weakness and/or disfiguring asymmetry | ||
| At rest: normal symmetry and tone | ||||
| Motion | ||||
| Forehead: none | ||||
| Eye: incomplete closure | ||||
| Mouth: asymmetric with maximum effort | ||||
| V | Severe dysfunction | Gross: only barely perceptible motion | ||
| At rest: asymmetry | ||||
| Motion | ||||
| Forehead: none | ||||
| Eye: incomplete closure | ||||
| Mouth: slight movement | ||||
| VI | Total paralysis | No movement | ||
Source: Adapted from House JW, Brackmann DE. Facial nerve grading system. Otolaryngol Head Neck Surg 1985;93:146–147. Reprinted with permission.
Pathogenesis
May20 suggested that Bell’s palsy begins with involvement of the sensory fibers of the facial nerve and subsequently involves the motor fibers. This process is consistent with the notion that the disease begins as a viral ganglionitis of the geniculate ganglion.21 Nasopharyngeal cultures,22 circulating antibodies,23 biopsy,24 polymerase chain reaction (PCR) of the geniculate ganglion from archived temporal bone,25 and PCR of intraoperative washings of the facial nerve26 from patients with Bell’s palsy all point to herpes simplex virus as the main etiologic agent. Ischemic and autoimmune injury have been proposed as the subsequent means of nerve degeneration, but it is now clear that entrapment at the meatal foramen and labyrinthine segment is critical in this process as originally described by Fisch and Esslen.27 The evidence for this includes the following:
1. Temporal bone histopathologic demonstration of a sharp demarcation between a normal nerve in the IAC and a severely degenerated nerve beyond the meatal foramen in a case of herpes zoster oticus6
2. Clear and convincing electrophysiologic evidence3,5 of conduction block at the meatal foramen and labyrinthine segment
3. Dramatic improvement in conduction across the labyrinthine segment after decompression3
4. Intraoperative observation at this institution and others10 of an edematous-appearing nerve in the IAC and a cadaveric-appearing nerve distally
5. Return of some facial movement in a small number of patients immediately after middle cranial fossa (MCF) decompression2
6. Clinical series demonstrating the efficacy of MCF decompression in cases of recurrent facial paralysis4,12
7. Gadolinium enhancement of the labyrinthine segment in Bell’s palsy and herpes zoster oticus (HZO)7–9,11,13
None of these data imply that MCF decompression is indicated for Bell’s palsy, but it has convincingly implicated the meatal foramen and labyrinthine segment in the pathologic process. Temporal bone morphometric evidence that the facial nerve is not as tightly constrained at the meatal foramen in young children may account for the lower incidence and better prognosis in this population.28
Prognosis
Several large studies have outlined the natural history of Bell’s palsy.29,30 Generally, patients older than age 65 at onset of idiopathic facial paralysis have a worse recovery of facial function than younger patients.29–31 Likewise, patients with diabetes not only have an increased incidence of Bell’s palsy but also have a poorer prognosis.30,31
The majority of patients have good recovery of facial function within 3 to 6 months without medical or surgical intervention (except, of course, eye care as needed). Identification of those patients who will not recover grade I or II function therefore should be the next goal after a diagnosis is made. Several important prognostic factors have been noted. Patients who never progress to complete paralysis and those with signs of recovery within the first 2 months have an excellent prognosis, with almost all returning to normal function. Electromyographic (EMG) evidence of voluntary activity32,33 or an intact stapedial reflex34 also portends an excellent prognosis. Finally, electroneurography (ENoG) findings of less than 90% degeneration of the electrically evoked compound muscle action potential during the first 2 weeks after onset of paralysis indicate almost certain near-normal or normal recovery. Patients with greater than 90% degeneration in the first 2 weeks have less than a 50% chance of good recovery.32,33,35 These patients should be the focus of aggressive treatment efforts.
Unfortunately, there is no electrophysiologic test that discriminates between nerve fibers that have undergone axonotmesis,36,37 which should recover fully, and those that have more severe injury.21 Further complicating this issue is intraoperative evidence of nerve fibers that are not stimulable distal to a pathologic process, but which become stimulable shortly after removal of the pathology. This represents injury more severe than neuropraxia, but clearly is not axonotmesis because the recovery is too fast to allow time for regeneration. This phenomenon may explain the rapid recovery reported after some MCF decompressions2 in which response to electrical stimulation was absent preoperatively. It is hoped that laboratory study of this process will improve clinical prognostication. For detailed discussion of prognostic electrical testing, see Chapter 9.
Eye Care
Eye care is the single most important treatment for any patient with grade II or worse facial function. Drying of the eye secondary to decreased eye closure and lacrimation rapidly leads to exposure keratopathy with breakdown of the cornea.38,39 To prevent this complication, artificial tears are applied at least every 2 hours during the day. At bedtime, ophthalmic ointment is applied and a moisture chamber of plastic wrap is used to cover the eye. Use of a temporary tarsorrhaphy, gold weight, or other oculoplastic techniques provides better eye protection when either facial nerve function is not expected to return or when exposure keratopathy cannot be prevented by medical treatment alone.38,39 Gold weights have almost entirely replaced tarsorrhapies.
Medical Treatment
Multiple placebo-controlled trials of glucocorticoid therapy for Bell’s palsy have demonstrated mixed results, with some studies demonstrating benefit and others showing none. For summaries of these studies with conflicting conclusions see Limb and Niparko,18 Selesnick and Patwardhan,40 and Salinas et al.41 For patients presenting within 3 weeks of onset of paralysis, we currently use prednisone 1 mg/kg/day for 14 days. Patients who have a medical contraindication to oral steroids are treated with weekly transtympanic injections of solumedrol 0.3 to 0.4 cc 40 mg/cc. Acyclovir treatment for Bell’s palsy is actively promoted by Adour et al,42 who claim a statistically significant benefit. However, a systematic review of this study and two other randomized controlled trials revealed a lack of consistent evidence for improved recovery from Bell’s palsy in patients treated with antivirals.43 Acyclovir has low toxicity and, as noted above, there are good theoretical reasons for its use. We currently treat patients with a 2-week course of valacyclovir in addition to steroids. A study by Murakami strongly supports antiviral treatments.26
Surgical Treatment
Surgical management of Bell’s palsy has evolved along with our understanding of the pathophysiology of the disease. May et al44 clearly demonstrated the futility of transmastoid decompression. Only MCF decompression of the meatal foramen, labyrinthine segment, and geniculate ganglion can be expected to offer any benefit. Although we perform the MCF approach frequently for acoustic neuroma and vestibular nerve section with minimal morbidity, it is technically challenging even for experienced temporal bone surgeons and has significant potential for complications. Thus, even with proof of the efficacy of decompression, we would only advocate its performance in centers experienced with the MCF approach.
Fisch’s45 landmark study of MCF decompression demonstrated statistically significant improvements in outcome with surgery, but it is difficult to assess the degree of improvement in this study. Use of the House-Brackmann scale in subsequent reports makes this much easier. All patients had >90% degeneration on ENoG within 14 days of onset of total paralysis and no voluntary EMG potentials. Fisch’s32 prognostic studies show at best a 50% rate of spontaneous “satisfactory” recovery when degeneration exceeds 90%. Sillman and coworkers33 studied ENoG prognostication using the House-Brackmann scale and verified Fisch’s result, demonstrating less than 50% recovery to grade I or II function when ENoG degeneration exceeded 90%. Thus the patients who would be expected to spontaneously return to grade I or II less than 50% of the time were treated with MCF decompression.
A multicenter prospective clinical trial of patients with Bell’s palsy showed that patients who did not reach 90% degeneration on ENoG within 14 days of paralysis (n = 54) all had return of function to House-Brackmann grade I or II (Table 28–2). Patients with ≥90% degeneration on ENoG and no EMG motor unit potentials were offered surgical decompression of the facial nerve through an MCF approach. Thirty-four elected to have the decompression, whereas 36 were managed with steroids only. The results of the comparison were statistically significant in favor of decompression (p < .0002 stratified exact permutation test). The surgical decompression group exhibited House-Brackmann grade I or II results in 91% of those undergoing MCF decompression within 14 days of onset of acute paralysis. Of the 36 patients who chose not to undergo surgical decompression and were treated solely with steroids, 58% had a poor outcome at 7 months follow-up (House-Brackmann grade III or IV). Only 9% of the patients who did have MCF facial nerve compression had a poor outcome (Table 28–2).46
Facial nerve decompression for Bell’s palsy is rarely necessary as severe degeneration is uncommon. However, when severe degeneration does occur within 14 days of the onset of acute paralysis, and there are no voluntary EMG motor units active, MCF surgical decompression is worthwhile.
| ENoG: ≥90% degeneration by 14 days | ||||
| EMG: no voluntary motor unit potentials | ||||
| House-Brackmann | MCF | Steroids | ||
| Grade | Decompression n | Only n | ||
| I | 14 | 5 | ||
| II | 17 | 10 | ||
| III | 2 | 19 | ||
| IV | 1 | 2 | ||
| I/II | 31(91%)* | 15(42%) | ||
| III/IV | 3(9%) | 21(58%) | ||
* p < .0002 stratified exact permutation test MCF, middle cranial fossa.
Management Algorithm
Our approach to management of Bell’s palsy is displayed in Fig. 28–2. We perform an ENoG when the patient has a total paralysis and is seen within the first 14 days. If the patient has nearly 90% degeneration or is degenerating quickly, frequent follow-up ENoGs are performed.32
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


