(1)
Department of Pathology, Duke University Medical Center, Durham, NC, USA
Abstract
The eyelids help protect the cornea, and they are vital for corneal health and transparency. For example, in cases of facial paralysis, failure to close the eyelids may result in corneal ulceration.
The eyelids are skin, and therefore, when you evaluate eyelid lesions, you are essentially practicing dermatopathology. Eyelid anatomy and histology is best studied on exenteration specimens or full-thickness eyelid excisional biopsies (Fig. 4.1).
Normal components of the eyelid include eccrine glands, apocrine glands of Moll (Fig. 4.2), sebaceous (meibomian) glands of the tarsal plate, and skeletal muscle fibers (levator muscle of the upper eyelid) (Fig. 4.3). The palpebral conjunctiva forms the posterior aspect of the eyelid.
Three eyelid lesions that tend to be more familiar to the ophthalmic pathologist are sebaceous carcinoma, chalazion (see Chap. 1), and phacomatous choristoma. This chapter will also introduce some of the other common lesions affecting the eyelid.
The eyelids help protect the cornea, and they are vital for corneal health and transparency. For example, in cases of facial paralysis, failure to close the eyelids may result in corneal ulceration.
The eyelids are skin, and therefore, when you evaluate eyelid lesions, you are essentially practicing dermatopathology.
Eyelid anatomy and histology is best studied on exenteration specimens or full-thickness eyelid excisional biopsies (Fig. 4.1). Normal components of the eyelid include eccrine glands, apocrine glands of Moll (Fig. 4.2), sebaceous (meibomian) glands of the tarsal plate, and skeletal muscle fibers (levator muscle of the upper eyelid). The palpebral conjunctiva forms the posterior aspect of the eyelid.
Three eyelid lesions that tend to be more familiar to the ophthalmic pathologist are sebaceous carcinoma, chalazion (see Chap. 1), and phacomatous choristoma. This chapter will also introduce some of the other common lesions affecting the eyelid.
Sebaceous Carcinoma of the Eyelid
Sebaceous carcinoma of the eyelid (also known as sebaceous cell carcinoma and sebaceous gland carcinoma) accounts for approximately 5% of all malignant eyelid tumors.
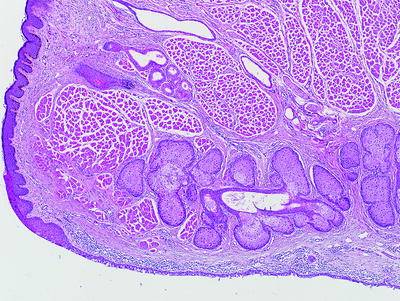
Fig. 4.1
Eyelid margin showing the epidermis and dermis with the orbicularis muscle, sebaceous glands of the tarsal plate, and the palpebral conjunctiva along the deep surface
It typically involves adults in the sixth and seventh decades of life.
These tumors arise from the cells (sebocytes) of the sebaceous glands of the eyelid including the meibomian glands (tarsal plate) and the Zeis glands (lash follicles).
Although the eyelids are a small percentage of the total skin content, this tumor seems to have a predilection for this location compared to the rest of the skin.
They are more common in the upper eyelid (possibly due to a higher concentration of sebaceous glands in the upper eyelid). Rare cases may initially present or arise in the conjunctiva, the caruncle, and the lacrimal gland.
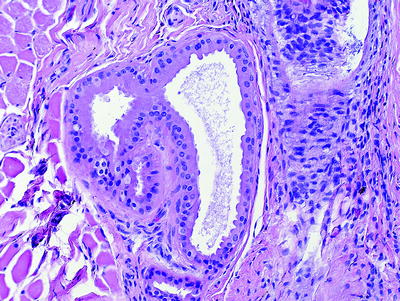
Fig. 4.2
Apocrine glands of Moll. The apocrine glands of Moll are a normal component of the eyelid dermis. Apocrine-related adenocarcinomas of the eyelid are rare tumors
Common presenting signs and symptoms include madarosis (loss of eyelashes), diffuse eyelid thickening, persistent keratoconjunctivitis or blepharitis, a caruncular mass, or a nodule resembling a chalazion. It is highly recommended that chalazia, especially “recurrent” ones, be submitted for histological examination.
Microscopically, sebaceous carcinoma is defined by cells with a characteristic lipid-rich and vacuolated cytoplasm (Fig. 4.3). This is not to be confused with the cytoplasmic clearing seen in clear cell carcinomas, either primary in the skin or metastatic (e.g., metastatic clear cell renal cell carcinoma.)
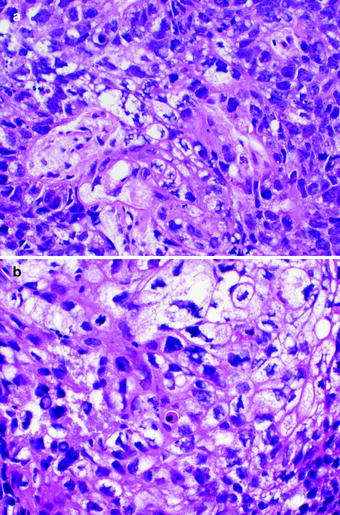
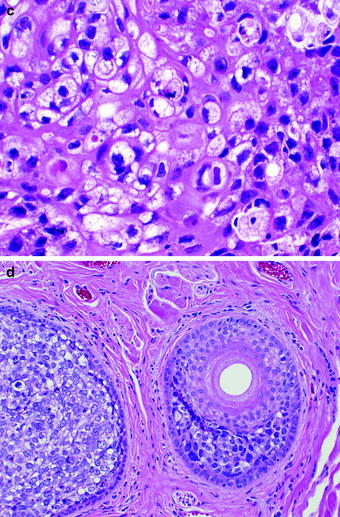
Fig. 4.3
a, b, c Sebaceous carcinoma is a malignant epithelial neoplasm of the eyelid. The cytoplasm of the tumor cells has a lipidized and vacuolated appearance. d Sebaceous carcinoma with periadnexal infiltration
Sebaceous carcinoma may exhibit marked cytological atypia (Fig. 4.4), and, in some cases, the tumor may be so poorly differentiated that the distinction between squamous cell carcinoma, basal cell carcinoma, a metastasis, or Merkel cell carcinoma might not be readily apparent. If frozen tissue is available, an oil red O stain will highlight the lipid and can be diagnostically helpful.
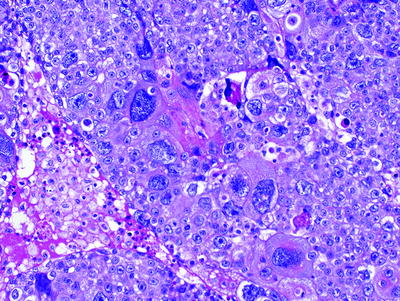
Fig. 4.4
Sebaceous carcinoma with marked cytological pleomorphism. Sebaceous morphology might not be obvious in poorly differentiated examples
Sebaceous carcinoma may undergo intraepithelial spread (Fig. 4.5) in a pagetoid manner as single cells, as nests of tumor cells, or as diffuse full-thickness involvement, beware of this when examining eyelid biopsies. A pattern of comedocarcinoma with central necrosis is also commonly seen (Fig. 4.6).
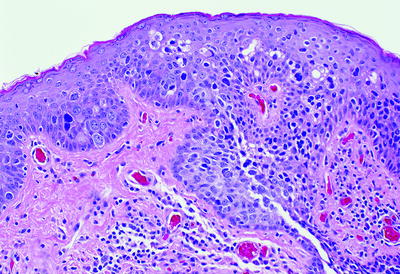
Fig. 4.5
Sebaceous carcinoma with intraepithelial/pagetoid spread
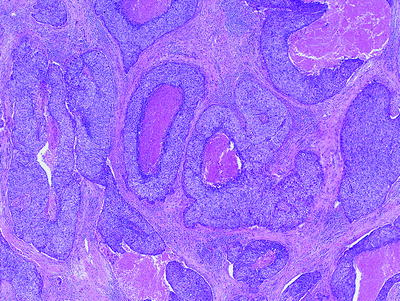
Fig. 4.6
Sebaceous carcinoma with a comedocarcinoma pattern with central necrosis
Sebaceous carcinoma may spread by direct or perineurial extension into the orbit, sinuses, and intracranially. Sebaceous carcinoma metastasizes via hematolymphoid channels to preauricular and cervical lymph nodes, the lungs (Fig. 4.7), liver, and brain.
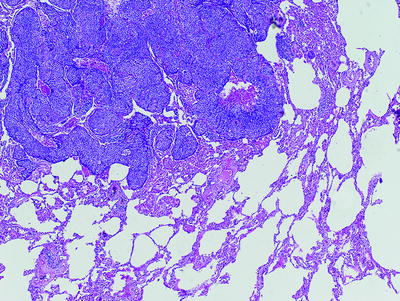
Fig. 4.7
Sebaceous carcinoma metastatic to the lung
By immunohistochemistry, sebaceous carcinomas are immunopositive to epithelial membrane antigen (EMA) (Fig. 4.8), Ber-EP4, and others including cytokeratin 7, Cam5.2, and BRST-1. EMA is typically negative in basal cell carcinoma, and Ber-EP4 is typically negative in squamous cell carcinoma; this profile can be helpful when attempting to determine if a poorly differentiated tumor is of sebaceous, squamous, or basal cell origin.
< div class='tao-gold-member'>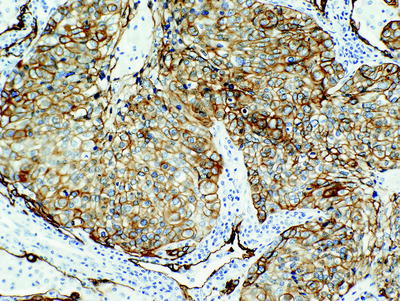 Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


