 Eyelid Hair Follicle Tumors
Eyelid Hair Follicle TumorsEyelid Trichoepithelioma
General Considerations
Trichoepithelioma is a benign tumor that can be solitary or multifocal (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16). Solitary trichoepithelioma is generally unassociated with genetic or systemic abnormalities. It can occur anywhere on the body, but has a predilection for the face and eyelids. The multifocal variant (Brooke’s tumor) is transmitted by an autosomal-dominant mode of inheritance. Trichoepithelioma accounts for about 1% to 2% of biopsied sweat gland or hair follicle tumors (10).
Clinical Features
Solitary trichoepithelioma generally has its onset in early adulthood as a skin-colored, dome-shaped papule that may remain stable or gradually enlarge and become crusty (1,2). Larger trichoepithelioma may have telangiectatic blood vessels and resemble basal cell carcinoma. However, unlike basal cell carcinoma, it is relatively stationary and rarely ulcerates (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15).
The autosomal-dominant multiple trichoepithelioma (also called Brooke’s tumor and adenoid cystic epithelioma) has its onset in the second decade of life and the lesions slowly increase in number (8). It begins as multiple, skin-colored, firm papules usually between 2 and 8 mm in diameter, located mainly in the nasolabial folds, facial skin, and sometimes the eyelids (7). Ulceration and transformation into basal cell carcinoma are rare. The clinical appearance may be similar to nevoid basal cell carcinoma syndrome, facial angiofibromas of tuberous sclerosis, sarcoidosis, or syringoma. Multiple trichoepitheliomas have also been observed in association with multiple cylindromas, a condition that also has autosomal-dominant inheritance (7,12,13). The gene for multiple trichoepitheliomas maps to chromosome 9p21 (16).
Pathology
Histopathologically, trichoepithelioma is characterized by irregular lobules of proliferating basal cells with distinct keratin cysts (horn cysts), that represent immature hair structures. The keratin cysts may resemble those seen with seborrheic keratosis or keratotic basal cell carcinoma and the tumor may be difficult to differentiate from basal cell carcinoma or squamous cell carcinoma in many instances. The keratin cysts can occasionally incite a foreign body giant cell reaction (7). Electron microscopy and immunohistochemical studies suggest that the tumor arises from hair matrix cells and the horn cysts represent attempts at hair shaft formation (7,8).
Management
Management is surgical excision (13,14,15). If an incisional biopsy confirms trichoepithelioma, definitive surgical removal can be done with less generous margins than for basal cell carcinoma, thus facilitating surgical reconstruction (15). The carbon dioxide laser has been used for multiple lesions (14). Multiple trichoepitheliomas are managed similarly; management varies with the clinical findings.
Selected References
1. Bishop DW. Trichoepithelioma. Arch Ophthalmol 1965;74:4-8.
2. Gray HR, Helwig EB. Epithelioma adenoides cysticum and solitary trichoepithelioma. Arch Dermatol 1963;87:102-114.
3. Wolken SH, Spivey BE, Blodi F. Hereditary adenoid cystic epithelioma (Brooke’s tumor). Am J Ophthalmol 1968;68:26-34.
4. Gaul LE. Heredity of multiple benign cystic epithelioma. Arch Dermatol 1953;68:517-519.
5. Simpson W, Garner A, Collin JRO. Benign hair-follicle derived tumours in the differential diagnosis of basal cell carcinoma of the eyelids: A clinicopathological comparison. Br J Ophthalmol 1989;37:347-353.
6. Rodgers IR, Jakobiec FA, Hidayat AA. Eyelid tumors of apocrine, eccrine, and pilar origins. In: Albert DM, Jakobiec FA. Principles and Practice of Ophthalmology. Philadelphia: WB Saunders; 1994:324-334.
7. Elder D, Elenitsas R, Ragsdale BD. Tumors of the epidermal appendages. In: Elder D, Elenitsas R, Jaworsky C, et al., eds. Lever’s Histopathology of the Skin. Philadelphia: Lippincott-Raven; 1997:751-755.
8. Font RL. Eyelids and lacrimal drainage system. In: Spencer WH, ed. Ophthalmic Pathology. An Atlas and Textbook. 4th ed. Philadelphia: WB Saunders; 1996:2313.
9. Bech K, Jensen OA. External Ocular Tumors. Philadelphia: WB Saunders; 1978:19.
10. Ozdal PC, Callejo SA, Codere F, et al. Benign ocular adnexal tumours of apocrine, eccrine or hair follicle origin. Can J Ophthalmol 2003;38:357-363.
11. Aurora AL. Solitary trichoepithelioma of the eyelid. Indian J Ophthalmol 1974;22:32.
12. Sternberg I, Buckman G, Levine MR, et al. Hereditary trichoepithelioma with basal cell carcinoma. Ophthalmology 1986:93:531-533.
13. Parsier RJ. Multiple hereditary trichoepitheliomas and basal cell carcinomas. J Cutan Pathol 1986;13:111-117.
14. Wheeland RG, Bailin PL, Kroanberg E. Carbon dioxide (CO2) laser vaporization for the treatment of multiple trichoepitheliomas. J Dermatol Surg Oncol 1984;10:470.
15. Votruba M, Collins CM, Harrad RA. The management of solitary trichoepithelioma versus basal cell carcinoma. Eye 1998;12:43-46.
16. Harada H, Hashimoto K, Ko MS. The gene for multiple familial trichoepithelioma maps to chromosome 9p21. J Invest Dermatol 1996;107:41-43.
Eyelid and Facial Trichoepithelioma
Trichoepithelioma can be solitary or multiple. In some instances, this benign tumor can spawn basal cell carcinoma (1,2).
Stemberg I, Buckman G, Levine MR, et al. Hereditary trichoepithelioma with basal cell carcinoma. Ophthalmology 1986:93:531-533.
 Figure 5.1. Solitary trichoepithelioma on lower eyelid in a 52-year-old man. (Courtesy of Ove Jensen, MD, and Knud Bech, MD.) |
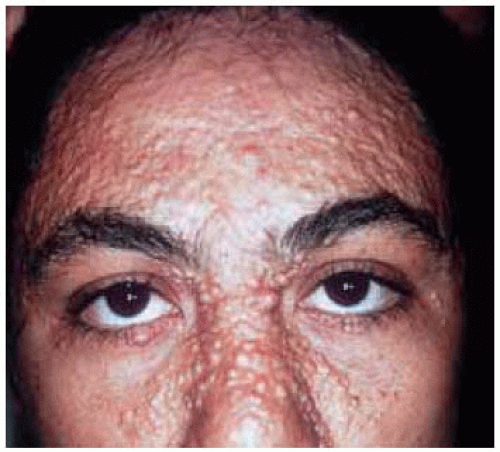 Figure 5.2. Young woman with multiple facial trichoepitheliom as (Brooke’s tumor). Three of her nine siblings had similar findings. (Courtesy of the Armed Forces Institute of Pathology, Washington, DC.) |
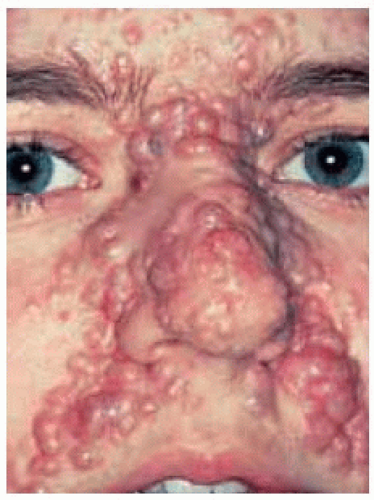 Figure 5.3. Young woman with multiple facial trichoepitheliom as (Brooke’s tumor). (Courtesy of Mark Levine, MD.) |
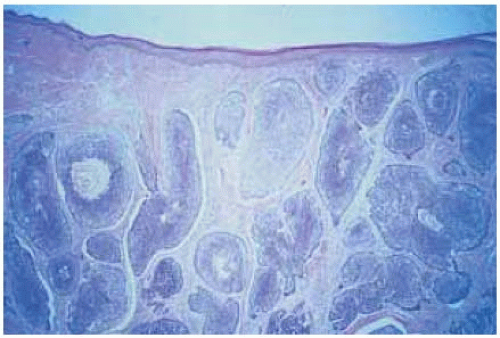 Figure 5.4. Histopathology of trichoepithelioma, showing deep tumor nodules with keratin cysts. (Hematoxylin-eosin 40.) (Courtesy of Mark Levine, MD.) |
 Figure 5.5. Photograph of the mother of the patient shown in Figure 5.3 showing similar lesions and a larger crusted tumor in the left medial canthus. This was excised and proved to be basal cell carcinoma arising in a patient with familial multiple trichoepitheliom a. (Courtesy of Mark Levine, MD.) |
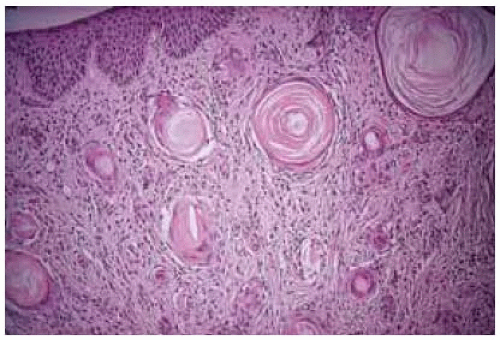 Figure 5.6. Histopathology of another case of trichoepithelioma, showing the well-defined keratin cysts. (Courtesy of the Armed Forces Institute of Pathology, Washington, DC.) |
Eyelid Trichofolliculoma and Trichoadenoma
General Considerations
Trichofolliculoma and trichoadenoma are similar hair follicle tumors that rarely affect the eyelids. Trichofolliculoma, a more common lesion than trichoadenoma, is a benign, slow-growing tumor of hair follicle origin that occurs most often in the head and neck region and can involve the eyelid (1,2,3,4,5,6,7,8,9). It accounts for about 1% to 2% of biopsied sweat gland or hair follicle tumors (3,4).
Clinical Features
Trichofolliculoma presents as a dome-shaped, skin-colored nodule with a characteristic central pore through which typical cotton-like fine hairs, sometimes white lanugo hairs, protrude. This is a highly diagnostic feature (1,2,3,4,5,6,7,8,9). In the ocular region, it has a predilection for the eyelid margin. Sebum-like material can intermittently drain from the pore. Clinically, it may be confused with sebaceous cysts, nevus, or basal cell carcinoma. Trichofolliculoma does not appear to have any systemic associations.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


