Eyelid Abnormalities: Ectropion, Entropion, Trichiasis
Kenneth V. Cahill
Marcos T. Doxanas
Numerous procedures have been described for the correction of lower eyelid abnormalities. These procedures are a reflection of the gradual evolution of operative approaches to the alleviation of underlying anatomic abnormalities. No longer are scarring procedures advocated. Specific anatomic defects are identified and rectified.
Thorough knowledge of eyelid anatomy is essential for the appreciation of the etiology and surgical intervention of lower eyelid abnormalities. The eyelid can be conceptualized to consist of an anterior and posterior lamella. The anterior lamella consists of the skin and orbicularis muscle. The thin delicate skin of the eyelid lacks the connective tissue, fat, and pilosebaceous apparatus of the dermis that would reduce eyelid mobility. The orbicularis muscle is categorized as either orbital or palpebral portions based on its association with underlying anatomic structures. The orbital orbicularis muscle overlies the orbital rim. The palpebral orbicularis muscle is further classified as preseptal or pretarsal based on the proximity of orbital septum or tarsus, respectively. At the eyelid margin a strip of orbicularis muscle, the muscle of Riolan, is directly associated with the eyelashes. This is responsible for the darker coloration of the slightly depressed midsection of the lid margin commonly referred to as the gray line.1
The posterior lamella consists of the eyelid retractor, the tarsus, and the conjunctiva. Hawes and Dortzbach2 reviewed and highlighted lower eyelid anatomy, specifically the lower eyelid retractor (Fig. 73-1). The lower eyelid is analogous to the upper eyelid; the main variation is the eyelid retractor system. The upper eyelid has a distinct eyelid retractor, the levator muscle, to enhance upper eyelid mobility. The lower eyelid does not have a specialized skeletal muscle eyelid retractor. The lower eyelid retractor system originates as a fascial extension of the inferior rectus muscle (capsulopalpebral head). This fascial system splits to encapsulate the inferior oblique muscle and then reunites to form a dense fibrous sheet (capsulopalpebral fascia) to insert onto the inferior tarsal border. The inferior tarsal muscle is a smooth muscle analogous to the superior tarsal muscle (Müller muscle) of the upper eyelid. This muscle originates in the inferior fornical area and extends toward the inferior tarsal border but does not insert on the tarsal border as its counterpart in the upper eyelid does. The inferior tarsal muscle receives sympathetic innervation, and interruption of its innervation will result in a slightly elevated position of the lower eyelid margin as observed in Horner syndrome. Otherwise, the inferior tarsal muscle has little pathologic significance.
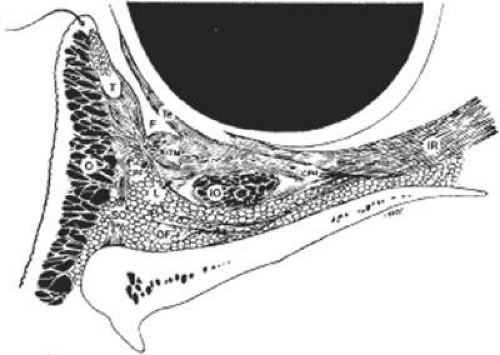 Figure 73.1. Sagittal section of the lower eyelid. The anterior lamella consists of the skin and orbicularis muscle (o). The posterior lamella consists of the conjunctiva, capsulopalpebral fascia (CPF), inferior tarsal muscle (ITM), and tarsus (T). F, fornix; Te, Tenon capsule; SO, septum orbitale; l, Lockwood ligament; IO, inferior oblique muscle; CPH, capsulopalpebral head; IR, inferior rectus; OF, orbital fat. (Reprinted with permission from Hawes JJ, Dortzbach RK: The microscopic anatomy of the eyelid retractors. Arch Ophthalmol 100:1313, 1982.) |
The tarsus provides the primary support or foundation for the eyelids. Although degeneration of the tarsus may promote eyelid laxity,3 the principle focus of weakness of the eyelids is at the lateral and medial canthal tendons.4 Jones and Wobig5 described the medial canthal tendon with a prominent anterior component firmly connecting the medial canthal angle to the maxillary process of the frontal bone. The posterior limb of the medial canthal tendon provides deep support with attachment to the posterior lacrimal crest. Anderson6 also emphasized the role of a superior branch of the medial canthal tendon to support the canthal angle. Gioia et al7 have provided a clear description of lateral canthal anatomy. The lateral canthal tendon has contributions from the lateral aspects of the tarsus and the preseptal and pretarsal orbicularis muscle; these insert on the inner aspect of the lateral orbital rim at the Whitnall (lateral orbital) tubercle. The posterior deep insertion of the lateral canthal tendon allows the lateral aspect of the eyelids to approximate the globe.
Ectropion and entropion share similar anatomic features. The most common predisposing anatomic factors for lower lid malpositions are horizontal eyelid laxity and weakness or defects of the lower lid retractors. The general weakness of the eyelid is caused by a weakness of the medial and lateral canthal tendons, permitting horizontal eyelid laxity.4 As such, it is best to consider lower eyelid laxity as resulting from laxity of the tarsoligamentous sling or support for the eyelid. The anatomic weakness can be demonstrated by the snap test. Downward retraction is exerted on the lower lid, pulling it away from the globe. On relapse, the lower lid should snap back against the globe spontaneously. Moderate laxity is present if a blink is necessary for the lid to return to its normal position. Failure of the eyelid to snap back against the globe with a single blink indicates excessive laxity of the tarsoligamentous sling.
The lower eyelid retractors may be weakened, stretched, or may actually become disinserted from the inferior tarsal border. Weakness or defect of the lower eyelid retractors creates instability of the inferior tarsal border that is manifested clinically as ectropion or entropion.
In addition, enophthalmos is associated with both ectropion and entropion. However, the role of enophthalmos as a pathophysiologic feature of lower eyelid malpositions has been grossly overstated.8,9,10 Enophthalmos may secondarily reduce tarsal stability by exaggerating horizontal lid laxity. It reduces the tension exerted on the eyelids by retraction of the globe and soft tissues. The normal arc or outward bowing of the eyelids is decreased with the enophthalmic globe, and eyelid tension is reduced. Retrobulbar injections may stabilize eyelid malpositions by reducing horizontal eyelid laxity. Volume introduced in the retrobulbar area re-establishes the normal outward arch, or bowing, of the eyelid.
The development of ectropion and entropion is a reflection of the relationship between the anterior and the posterior lamellae. The eyelid position is maintained by an appropriate balance of the anterior and posterior lamellae. If tractional forces are unbalanced, eyelid malpositions may manifest as ectropion, entropion, or eyelid retraction. If vertical traction is produced by the anterior lamella, either by chronic cicatricial changes or mechanical aberrations, the eyelid margin is retracted inferiorly or is everted away from the globe. This most commonly results from mild solar-induced changes, dermatitis that tightens the skin of the eyelids and face, and following surgical procedures or trauma of the eyelid, which produce a shortening or scarring of the skin and underlying orbicularis muscle.
Involutional entropion is more complex because of the multitude of factors producing this abnormality. The tarsal instability of entropic lids is owing to horizontal eyelid laxity and loss of support of the lower eyelid retractors.11 The orbicularis muscle dynamics also assume a prominent pathophysiologic role in the production of entropion. In entropic eyelids, the preseptal orbicularis muscle overrides the pretarsal orbicularis muscle, which rolls the superior border of the tarsus internally. This is differentiated from spastic entropion, which is theoretically owing to a spasm of the Riolan muscle. However, the primary differentiating feature of spastic entropion is a specific precipitating etiologic factor, such as recent eye surgery, eyelid edema, or ocular inflammation with secondary eyelid edema. An appreciation of the multiple etiologic causes of entropion has resulted in the evolution of combined approaches to correcting the various anatomic abnormalities and stabilizing the tarsus and orbicularis muscle.12,13,14,15
This chapter is divided into three sections that discuss eyelid abnormalities. These include ectropion, entropion, and trichiasis. Sections on ectropion and entropion are further divided according to the underlying cause of the eyelid malposition. Specific surgical approaches are highlighted in each section.
ECTROPION
Ectropion is an eversion of the eyelid away from the globe. It is classified according to its anatomic features as involutional, cicatricial, tarsal, congenital, or paralytic (Fig. 73-2). Surgical approaches can be directed toward the underlying etiologic factors.
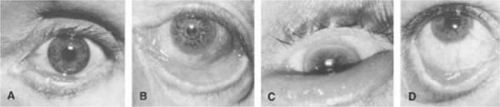 Figure 73.2. Clinical presentation of ectropion. A. Medial ectropion. B. Generalized ectropion with retraction of eyelid. C. Tarsal ectropion, with total eversion of tarsus. D. Cicatricial ectropion developing following orbital floor exploration. |
INVOLUTIONAL ECTROPION
Involutional ectropion evolves slowly secondary to eyelid laxity and tractional forces of the anterior lamella. This may result from mild cicatricial changes of the skin or orbicularis muscle or a mechanical or gravitational eversion of the eyelid margin. There is generally a progression from eyelid laxity to punctal ectropion, medial ectropion, and then generalized ectropion. If the punctum is slightly everted from the lacus lacrimalis, tears cannot effectively drain into the canalicular system. In addition, the siphoning effect of the lacrimal excretory system, as demonstrated by Doane,16 is not generated if the lacrimal puncta do not occlude on lid closure and do not approximate the lacus lacrimalis. With the puncta approximated, attempted eyelid opening creates negative pressure within the lacrimal excretory system. When the puncta initially separate, the negative pressure siphons tears from the lacus lacrimalis. Also, horizontal eyelid laxity may produce a flaccid canalicular syndrome or poor lacrimal pump, so that tears are not siphoned from the lacus lacrimalis.17 This tearing malfunction is aggravated by the chronic ectropion and eyelid retraction that produce lagophthalmos and secondary exposure keratopathy. With time, the exposed conjunctiva thickens and keratinizes, producing further ocular irritation.
Mild medial ectropion is manifested by rotation of the punctum away from the ocular surface, causing mild tearing. This can be treated with a one- or two-snip punctal plasty, establishing anatomic continuity between the canalicular system and lacus lacrimalis in the medial canthal angle. This procedure is performed by opening the punctum and vertical canaliculus with a single snip of a sharp iris or Westcott scissors or by excising a very thin “V” wedge (two snips). This procedure may also be helpful after ectropion repairs if a mild punctal eversion remains. This can be performed as an office procedure. A cotton-tipped applicator saturated with 4% lidocaine solution held over the punctum and adjacent palpebral conjunctiva usually provides adequate anesthesia. If it does not, a 30-gauge hypodermic needle can be passed through the punctum and vertical canaliculus so that 1% or 2% lidocaine is infiltrated into the pericanalicular tissue. Medial ectropion, when more severe, may require surgical intervention. Surgery directed at the lateral canthal angle, as discussed later in this chapter, does not fully alleviate medial lid malpositions, and this approach is not universally successful in restoring eyelid position. Removal of a conjunctival and lower lid retractor spindle may be necessary. The spindle is directly beneath the tarsus with its long axis directly parallel to the eyelid margin (Fig. 73-3). The conjunctival retractor spindle should measure no more than 5 mm in a vertical dimension to prevent postoperative retraction and entropion resulting from posterior lamellar shortening. In essence, the closure of this internal lamellar resection creates a direct tightening of the medial lower lid retractors. Full-thickness lid sutures tied over a firmly rolled cotton or silicone bolster have been described by Collin.18 Although this technique is a short-term nuisance for the patient, it does result in a superior inward rotation of the punctum and lid margin without retraction.
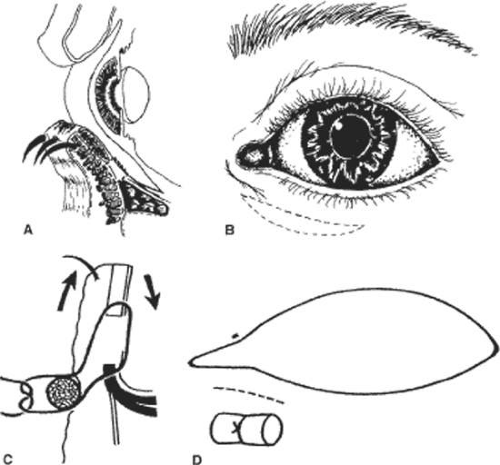 Figure 73.3. Conjunctival lower lid retractor spindle removal. Medial ectropion can be repaired by removal of a conjunctival lower lid retractor spindle from the medial eyelid. (A, cross-sectional view; B, frontal view). A full-thickness suture closure with one or more 5-0 sutures tied over an external bolster of firmly rolled cotton or silicone sponge not only closes the resection of conjunctiva and the lower lid retractors but also advances upward the anterior lamella, increasing the inversion of the punctum. (C, cross-sectional view; D, frontal view). (Reprinted with permission from Collin JROC: A Manual of Systematic Eyelid Surgery. Edinburgh: Churchill Livingstone, 1982:31.) |
For cases of prominent medial ectropion, the Byron Smith19 “Lazy T” procedure combines a horizontal lid-tightening procedure with a lower lid retractor resection. This combined procedure inverts the eyelid margin to its appropriate anatomic position. Full-thickness eyelid resections and repairs have been poorly demonstrated and reported in the ophthalmology and plastic surgery literature. The concept of a wedge resection or pie-shaped tarsal resection should be totally discarded. In its place, full-thickness modified pentagonal block resections should be used (Fig. 73-4). Incision through the eyelid should be perpendicular to the lid margin. If the eyelid resection is wedge shaped, the repair or approximation of the lid results in a notch or valley of the eyelid margin at the incision site. The layered repair of the lid margin defect should start with approximation of the tarsus. Adequate tarsal approximation provides the foundation for lid reconstruction and removes all tension from the eyelid margin. As a result, lid notches or trichiasis should be almost nonexistent.
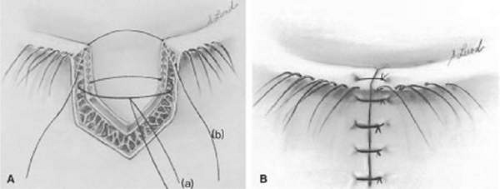 Figure 73.4. Pentagonal block eyelid resection. A. Tarsal approximation provides the foundation for eyelid closure. PDS suture is used to approximate the base of the tarsus (suture a). The lid margin is closed by a suture angled from the eyelid margin (suture b). B. Sutures at the eyelid margin are totally without tension and are generally of 6-0 or 7-0 silk. |
The initial interrupted sutures should be placed through the base or inferior border of the tarsus to promote tension-free lid approximation Fig. 73-4A, suture a). The first suture for tarsal approximation is a 5-0 or 6-0 polydioxanone (PDS) or polyglactin (Vicryl) with a spatula-style needle. If prominent lid tension is evident, a 5-0 suture is preferable. The PDS is an absorbable suture that retains its tensile strength for 6 weeks and promotes little tissue reaction. Vicryl is also an absorbable suture that retains its tensile strength for 3 to 4 weeks. It is more prone to cause tissue reaction in some patients. Horizontal approximation of the cut edges of the lower lid retractor with interrupted 6-0 PDS sutures may also help to reduce horizontal lid tension. Continuous running sutures through the lower lid retractors from the inferior aspect of the modified pentagonal lid resection to the base of the tarsus result in a downward traction of the eyelid resulting from vertical shortening of the lid retractors and should be avoided.20 To avoid a suture that is tied at the lid margin, a superior tarsal suture is initiated on the anterior tarsal surface approximately 2 mm from the cut edge of the tarsus and 2 mm inferior to the lid margin (Fig. 73-4A). The suture is then angled to exit the cut surface of the tarsus adjacent to the posterior lid margin. The opposing suture is then placed in a mirror image fashion from the posterior lid margin to exit the tarsus at 2 mm from its cut edge and 2 mm from the lid margin. Tying this suture approximates the lid margin perfectly and establishes an appropriate foundation for its repair. Additional sutures of 6-0 or 7-0 silk can be placed directly anterior and posterior to the lashes to further stabilize the lid margin (Fig. 73-4B). Silk sutures tied as a square knot are used at the lid margin because they do not unravel and abrade the cornea. The skin is closed with a nonabsorbable polypropylene (Prolene) or nylon suture or an absorbable 6-0 gut (Ethicon 1916).
The Byron Smith Lazy T procedure creates a horizontal and vertical tightening of the nasal aspect of the lower eyelid. Modifications of the procedure as originally described by Smith are warranted. Smith originally described the removal of a tarsal conjunctival ellipse as the initial step in the procedure. In addition, he later described a wedgelike resection of the tarsus in the second stage of the procedure. We have found the procedure to be much easier to perform by initially resecting a full-thickness pentagonal block from the nasal portion of the eyelid. The initial incision with a sharp iris scissors should be perpendicular to the eyelid margin 3 to 4 mm lateral to the punctum extending to the base of the tarsus (Fig. 73-5A). The second side of the inferolaterally through the full-thickness eyelid. The lid margins are then grasped with forceps and overlapped to determine the amount of horizontal eyelid laxity. After marking the amount of eyelid laxity, the sharp iris scissors are used to complete the modified pentagonal block resection (Figs. 73-5B and C). The conjunctiva and adjacent lower eyelid retractors are incised at the base of the tarsus and extended nasally (Figs. 73-5E and F). After adequate undermining, the conjunctiva and lower eyelid retractor is overlapped, and a wedge or triangle of tissue is removed. The cut edge of the lower eyelid retractor and conjunctiva is then sutured to the inferior tarsal border using 6–0 chromic sutures, with the knots buried or directed away from the conjunctival surface to prevent ocular irritation (Fig. 73-5G). Alternatively, a full-thickness lid suturing technique tied over an external bolster may be used as previously described. After repair of the conjunctival lower lid retractor resection, the full-thickness eyelid resection is repaired as previously described.
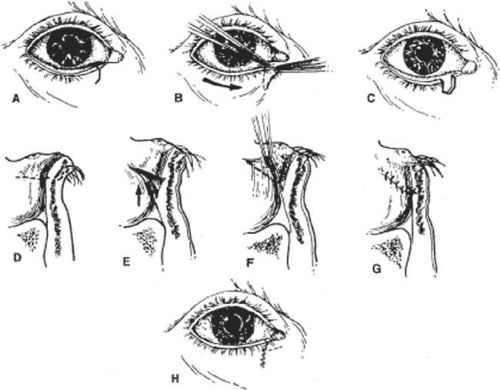 Figure 73.5. Byron Smith Lazy T procedure. Pentagonal block resection of the medial eyelid (A–C), followed by removal of a conjunctival lower eyelid retractor triangle in the medial eyelid (D–G). Suture knots are buried to prevent conjunctival irritation (G). H. Final schematic demonstrating site of lower lid full-thickness pentagonal resection and conjunctival lower lid retractor removal. |
Prominent laxity of the medial canthal tendon presents a challenge in management because of the deep fixation of the tendon and difficulties in obtaining a patent functional canalicular system.21,22 Fortunately this condition is rarely encountered. When past trauma or extreme involutional changes necessitate recreation of the deep attachment of the medial canthal tendon to the posterior lacrimal crest, microplate fixation may be a helpful technique.23 Attempts to plicate the anterior aspect of the medial canthal tendon at its insertion to the anterior lacrimal crest may result in kinking or folding of the canalicular system. To alleviate canalicular and medial canthal laxity, a block resection can be performed in the medial canthal angle that includes the medial canthal tendon and the canaliculus. The canaliculus is intubated with silicone, and the deep extension or insertion of the medial canthal tendon is reapproximated. In this fashion, the canalicular system remains patent and functional. In patients with a nonfunctioning lacrimal excretory system, Jordan et al24 have described a medial tarsal strip procedure to elevate and tighten the medial aspect of the lower eyelid. If the medial lower lid is lax and has a nonfunctioning canaliculus resulting from an inadequately repaired trauma, the block resection technique with canalicular intubation and reanastomosis offers a means of improving lid position and function, as well as the possibility of restoring lacrimal drainage.
If ectropion is generalized, lid-tightening procedures are advocated. Traditionally, lid-tightening procedures have consisted of horizontal shortening of the tarsus to permit better eyelid approximation. The original Kuhnt-Szymanowski procedure involved splitting the eyelid margin at the gray line and shortening the posterior lamella of the lid. This avoided a full-thickness lid resection with its associated difficulties in suture techniques and wound approximation. Smith19 later modified the technique to include a full-thickness resection of the eyelid, and this was the preferred procedure for ectropion repairs for many years. Unfortunately, this procedure involves the resection of normal tarsus and results in a narrowed palpebral fissure and possibly trichiasis and notching resulting from inadequate lid margin approximation.
Tenzel et al25 and Anderson and Gordy26 suggested directing attention to the lateral canthal tendon, with the lateral canthal sling and lateral tarsal strip procedures, respectively. The ease in performing the tarsal strip procedure has made it the preferred technique directed at the lateral canthal angle. Tightening at the lateral canthus restores the deep fixation of the lateral eyelid to the inner aspect of the orbital rim. In the enhanced tarsal strip procedure,27 reapproximation of the lateral eyelid corrects increasing degrees of cicatricial ectropion. In this procedure a full-thickness lateral aspect of the lid is sutured to the inner aspect of the lateral orbital rim. Advantages of the tarsal strip procedure include direct repair of the anatomic defect, no eyelid margin sutures near the cornea, preservation of the normal tarsus, avoidance of horizontal eyelid tissue shortening, simultaneous repair of canthal malpositions, and maintenance of lateral canthal contour.
The tarsal strip procedure has multiple uses in lower eyelid surgery, including involutional and cicatricial ectropion and entropion (Fig. 73-6). Appreciation of subtle anatomic features (as previously described) of the lateral canthal area greatly facilitate this procedure.7 The lateral tarsal strip procedure can be confined to the lateral canthal area, or an infralash incision can be extended to permit identification of lower eyelid anatomic features and removal of redundant skin and muscle. A lateral canthotomy is performed with a sharp iris scissors (Fig. 73-6A). The attached inferior crus of the lateral canthal tendon prevents mobilization of the lateral canthal angle. To incise the inferior extension of the tendon, the scissors should be directed inferior and nasally (Fig. 73-6B). Once the inferior crus of the tendon is incised, the lateral aspect of the eyelid is fully mobile. A free tarsal strip is created by denuding the tarsus of the eyelid margin, orbicularis muscle, lower eyelid retractor, and conjunctiva (Fig. 73-6C). Reattachment of the tarsal strip to the periosteum is a potential source of complications. Guidelines should be observed to prevent dystopias of the lateral canthal position. A horizontal plane should be established from the medial canthal angle to midpupil of the eye in primary gaze. The tarsal strip should be attached to the periosteum respecting this horizontal plane. In addition, the tarsal strip should be attached to the inner aspect of the lateral orbital rim, simulating attachment to the Whitnall (lateral orbital) tubercle (Fig. 73-6D). If the tarsal strip is attached to the anterior aspect of the lateral orbital rim, the deep or posterior forces of the lateral aspect of the eyelid are deficient. As a result the lateral eyelid does not approximate the globe. To further promote posterior forces, the tarsal strip should be reapproximated to the inner aspect of the lateral orbital rim by interrupted sutures tied on the anterior tarsal surface. Attempts to bury sutures beneath the tarsus are counterproductive because they promote elevation of the tarsal strip from the lateral canthus. The lateral canthal angle is reformed with a buried 6-0 PDS or Vicryl suture to restore perfect lateral canthal angle architecture (Fig. 73-6E).
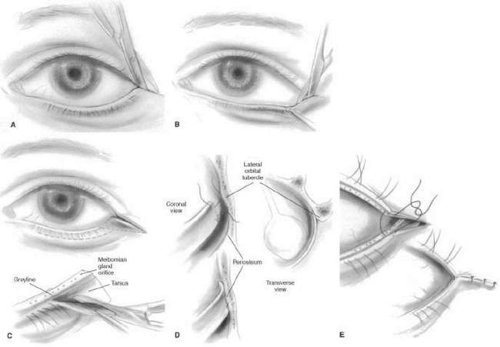 Figure 73.6. Tarsal strip procedure. A. Lateral canthoplasty. B. Lysis of inferior crus of lateral canthal tendon mobilizes the lateral aspect of the eyelid. C. Creation of denuded lateral tarsal strip. D. Approximation of the lateral tarsal strip to the inner aspect of the lateral orbital rim with two interrupted 5-0 Prolene sutures. E. Re-creation of the lateral canthal angle with absorbable suture, preventing lateral canthal angle malpositions. |
Complications of the lateral tarsal strip procedure primarily involve reattaching the tarsus to the periosteum at the inner aspect of the lateral orbital rim. Concerns regarding adequate fixation of the tarsal strip have already been addressed. It is not unusual, however, to have persistent tenderness at the lateral canthal angle until the normal inflammatory response gradually resolves. Occasional persistent lower lid edema can complicate the postoperative course.
CICATRICIAL ECTROPION
Cicatricial ectropion is the result of a shortening of the anterior lamella of the eyelid. This can result from excessive sun exposure, burns, radiation, or dermatitis, but is often the result of surgical treatment of the lower eyelids.
Surgeons are often alarmed at the precarious status of the lower lid and how it may be altered by surgical interventions such as blepharoplasty, tumor excision, or orbital floor exploration. Minimal or no skin excision may result in eyelid malpositions such as lid retraction or ectropion, because surgical undermining of skin or orbicularis muscle may result in some tightening during the healing phase. Shorr and Seiff28 explained this phenomenon as resulting from contracture of the middle lamella of the eyelid, the orbital septum. The orbital septum is a multilaminated structure29 that is relatively immobile and if scarred may lead to lower eyelid retraction or frank ectropion. According to Shorr, scarring of the orbital septum is a source of eyelid malpositions following explorations of the lid in which no skin is excised or following blepharoplasties with minimal skin excision. These changes are particularly prevalent in horizontally lax eyelids. A snap test as previously described should be performed on all patients undergoing lower eyelid surgery. If excessive laxity exists, eyelid-tightening procedures (tarsal strip) should be coordinated with the primary procedure to minimize postoperative eyelid malpositions.
The concept of internal scarring and horizontal lid laxity as etiologic factors in cicatricial ectropion is of paramount importance in the management of this disorder. Skin grafting should be restricted to those patients with severe cicatricial changes. Most cases of moderate ectropion are managed by a tarsal strip procedure or a Smith modification of the Kuhnt-Szymanowski procedure, in which a skin muscle flap is created but no skin is removed. Jordan and Anderson27 have advocated the enhanced tarsal strip procedure as an alternative to skin grafting. The lateral aspect of the lid is immobilized in this procedure, but no skin is excised as in the traditional tarsal strip procedure. The full-thickness lateral aspect of the eyelid is then approximated to the inner aspect of the lateral orbital rim. The firm deep attachment of the skin provides a sharp lateral canthal angle and supports tension from the anterior lamellar shortening.
If the procedures described previously prove ineffective in the management of cicatricial ectropion, a full-thickness skin graft is the final alternative (Fig. 73-7). Split-thickness grafts should be avoided in eyelid reconstruction because of graft scarring and contracture producing a pale immobile eyelid. Split-thickness grafts are effective in extensive tumor resections in which grafts are placed on avascular areas such as bone. The use of full-thickness skin grafting to the lower eyelid often must be accompanied by additional horizontal lid tightening (Fig. 73-7C). Suitable skin graft donor sites include the upper eyelid, preauricular or postauricular areas, and the supraclavicular areas. The skin graft should be carefully thinned and debrided of connective tissue to enhance graft survival. Localization and mobilization of the orbicularis muscle to provide a vascular bed also promotes graft survival and produces a more natural-appearing eyelid.30 The eyelid is immobilized by a superior traction suture or temporary suture tarsorrhaphies. A compressive bolster tied over the graft remains in place for 5 to 7 days.
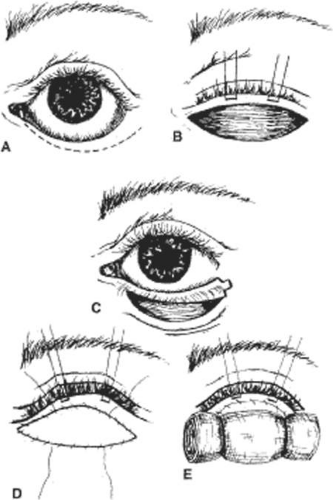 Figure 73.7. Cicatricial ectropion: skin grafting. A. Ectropion secondary to anterior lamella shortening. B. Elevation of the lower eyelid. Note that orbicularis muscle provides a vascular bed for the skin graft. C. Lateral tarsal strip may be required to horizontally tighten the lower eyelid before placement of the skin graft (D and E). |
In some cases of cicatricial ectropion, the anterior lamellar deficiency may be at least in part the result of a descent (sagging) of the midface. Depending on the goals of the patient, the need for full-thickness skin grafting may be decreased or even eliminated by surgical techniques that advance the midface soft tissue upward.31
TARSAL ECTROPION
Tarsal ectropion is an unusual form of ectropion produced by a disinsertion of the lower lid retractors, the capsulopalpebral fascia, from the inferior tarsal border32,33,34 (Fig. 73-8A). It is characterized by a total eversion of the tarsus. The inferior tarsal border may be positioned as high as the level of the inferior limbus. Defects of the lower lid retractors are most often associated with involutional entropion. However, in patients with tarsal ectropion the tractional forces from the anterior lamella will evert the entire tarsus. Indications of a defect in the lower lid retractors in these patients include (i) a deep inferior fornix, (ii) a higher-than-normal resting position of the lower eyelid, (iii) a diminished lower lid excursion, and (iv) direct visualization of the disinsertion through the conjunctiva. A prominent bulge of orbital fat can sometimes be seen in the area of the disinserted lower lid retractors when the lower lid is pulled down while the patient looks upward.
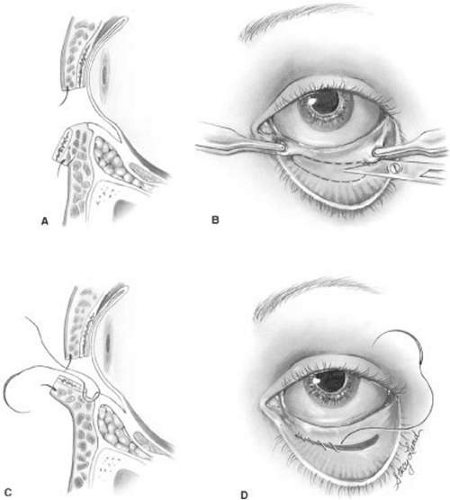 Figure 73.8. Tarsal ectropion. A. Ectropion secondary to disinsertion of the lower lid retractors. B. Everted lower eyelid and the area to be excised. C and D. Resected conjunctival spindle and reapproximation of the lower eyelid retractors. (Reprinted with permission from Wesley RE: Tarsal ectropion. Am J Ophthalmol 93:491, 1982.)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|