24 Extended Endonasal, Endoscopic Transsphenoidal Approach versus Craniotomy for Giant Pituitary Macroadenomas
With the exception of medically treatable prolactinomas, surgery is the first-line treatment for symptomatic giant pituitary adenomas. The surgical treatment for giant pituitary macroadenomas has evolved considerably over the past 100 years including the development of the transsphenoidal approach, extended transsphenoidal approach, endoscopic endonasal skull base techniques, and advances in transcranial and open skull base techniques. Either transcranial or transsphenoidal techniques can be employed for the treatment of giant pituitary macroadenomas; sometimes both approaches have been used either simultaneously or in a staged fashion.1–7 The goals of surgical treatment include improvement of visual function, endocrinologic function, and neurologic symptoms. Maximizing the extent of resection in the setting of a low morbidity and mortality rate is also a goal of surgery.
The surgical outcome in cases with giant pituitary adenoma have generally been reported to be poor because of a high rate of surgical morbidity secondary to small vessel ischemia of the hypothalamic walls and brainstem.8–10 A partial or subtotal resection can lead to infarction and edema of the residual tumor, in turn leading to postoperative neurologic deterioration.5,11 The high mortality rate during the early macrosurgical experience with transcranial surgery for pituitary tumors in general led to development of extracranial approaches to the sella.12,13 The transsphenoidal approach quickly became the most widely adopted technique, and the transcranial approaches were often reserved for giant pituitary macroadenomas with complex extensions into the retrochiasmatic region, ventricular system, and anterior or middle fossa.10,14,15 However, with recent introduction of endoscopic endonasal techniques for access to the ventral skull base and the suprasellar cisterns, the indications for transcranial and transsphenoidal surgery are once again being redefined.16–20
 Definition of Giant Macroadenomas
Definition of Giant Macroadenomas
The definition of a giant pituitary macroadenoma has been somewhat arbitrary. Using pneumoencephalography Hardy classified tumors as follows: type A, tumor that is bulging into the chiasmatic cisterns; type B, tumor that reaches the floor of the third ventricle; type C, large suprasellar tumor growth into the third ventricle up to the foramen of Monro; and type D, tumors that extend into the anterior or middle cranial fossa.21 This classification was then modified to incorporate modern computed tomography (CT) and magnetic resonance imaging (MRI). The suprasellar extensions of macroadenomas were graded, and the giant tumors were considered to be grades C and D. Grade C included tumors with large suprasellar extensions up to 3 cm filling the anterior third ventricle, and grade D were either huge tumors with >3 cm suprasellar extension above the foramen of Monro or a grade C tumor with asymmetrical or multiple lateral extensions.9 The critical threshold was a superior tumor margin greater than 2 cm above the jugum sphenoidale.9 However, these classifications consider the tumor from the transsphenoidal approach.
Symon et al15,22 defined giant pituitary tumors as those with suprasellar extensions over 4 cm above the jugum sphenoidale and that had less than 6 mm from the highest point of the tumor to the foramen of Monro. Not all giant pituitary adenomas extend into the third ventricle, and other studies have limited them to tumors over 3 or 4 cm in diameter regardless of the direction of growth.23,24 In general, the extrasellar extension of a giant pituitary adenoma can occur in any direction.10 Yasargil25 incorporated elements of these classification schemes and classified giant pituitary adenomas as tumors that extend out of the sella in any direction and divided them into four subgroups: (1) suprasellarsuprachiasmatic: tumors that grow in front of the chiasm with greater than 2 cm above the planum sphenoidale; (2) suprasellar-retrosellar: tumor growth behind the chiasm filling the interpeduncular cistern and into the third ventricle or the prepontine cistern; (3) parasellar-cavernous: tumor growth laterally into the cavernous sinus or into the middle fossa; and (4) paninvasive: tumor invading in all directions retrochiasmatic, epidurally into the middle fossa and prepontine cistern.
 Transcranial Surgery for Giant Macroadenomas
Transcranial Surgery for Giant Macroadenomas
Horsley26 is credited with performing the first successful resection of a pituitary tumor in 1889. He then used a subfrontal and middle fossa approach with a mortality rate of 20% in 10 patients between 1904 and 1906. At the same time Krause27,28 removed a pituitary tumor using a mostly extradural subfrontal approach in 1905. McArthur29 incorporated removal of the supraorbital ridge and orbital roof to expose a pituitary tumor in 1908. Frazier30,31 shifted to an intradural frontobasal approach and considered it superior to the transsphenoidal approach in patients with visual disturbances. These techniques were later modified by Cushing,32 Dandy,3 and Heuer,33 and a large experience with transcranial surgery for pituitary tumors was developed.34–36 With development of microsurgical techniques to open the sylvian fissure and refinement of the pterional approach with sphenoid wing removal, Yasargil et al37 described an unobstructed direct view to the parasellar structures. The shift from macrosurgical approaches to microsurgical approaches in the 1970s dramatically reduced the morbidity and mortality of transcranial surgery for giant pituitary adenomas.10,15,38 Variations of these approaches were then introduced depending on the extension of the tumor laterally, into the suprasellar space, into the third ventricle, and to minimize brain retraction (orbitozygomatic, interhemispheric transcallosal, and frontobasal interhemispheric approaches).25,37,39–45
As the transsphenoidal approach gained in popularity, these transcranial approaches were eventually reserved for (1) pituitary tumors with extension into the anterior, middle, or posterior fossa; (2) hourglass-shaped tumors presumably with a small diaphragmatic hiatus; (3) presence of a suprasellar tumor in the setting of a small sella; and (4) fibrous tumors that proved too difficult to remove from a transsphenoidal approach.5,38,46 Other indications for a transcranial approach include an active sinus infection in a patient for whom surgical delay poses the threat of acute neurologic deterioration; the presence of dolichoectatic internal carotid arteries that meet in the sella, that is, “kissing” carotid arteries; persistent visual loss after incomplete resection via the transsphenoidal route; and loss of occulomotor function.45,47
The operative mortality after transcranial surgery for giant pituitary adenomas was unacceptably high in the macrosurgical era, ranging from 18 to 33% in the acute post-operative period.34,48–51 In one retrospective review with 16 cases of giant pituitary macroadenomas there was an 18% acute operative mortality rate associated with a 61% rate of radical excision, with one patient having a transient postoperative visual deterioration.15 Microsurgery and experience dramatically lowered the operative mortality rate, which trended from 30% in 1953–1972 to 10% in 1973–1977 and to 6% in 1978–1983.10 Unfortunately, the literature regarding transcranial approaches to giant pituitary macroadenomas is heterogeneous without clear selection criteria for a surgical approach and with variable data regarding the extent of resection.
The use of the microsurgical technique in combination with traditional transfrontal or transtemporal approaches to giant pituitary adenomas led to a substantial reduction in operative mortality. In one surgical series of 21 patients with giant pituitary adenomas measuring >4 cm in diameter, there was only one postoperative mortality secondary to renal failure and no postoperative cerebrospinal fluid (CSF) leak, worsening of vision, or reported diabetes insipidus (DI). Six patients had prolactinomas and 10 patients had evidence of hypopituitarism before surgery. Postoperatively, seven patients had improvement in their endocrinologic and ophthalmologic symptoms, and the rest were unchanged. However, a radical excision was not achieved in any of the 21 patients52 (Table 24.1). In contrast, in a series of 319 patients with pituitary adenomas, there were 21 patients with giant adenomas (the authors define giant adenomas vaguely as adenomas with massive suprasellar extension) who underwent transcranial tumor resection with a subfrontal pterional approach.53 The increased gross total resection rate that was achieved in eight patients (38%) was associated with a 10% (two patients) operative mortality. Postoperative worsening of visual function occurred in two (9.5%) patients, and none of the patients had evidence of CSF leak. Postoperative DI occurred in four patients (19%). All 21 patients had marked hypopituitarism on presentation, and 10 (48%) demonstrated improvements in anterior pituitary function after surgery (Table 24.1). It is unclear to what degree the growth hormone/insulinlike growth factor (GH/IGF) levels were normalized in the three patients with GH-secreting giant adenomas.53
In a separate series of 26 patients who underwent transcranial surgery and 85 patients who underwent transsphenoidal surgery for giant pituitary adenomas (>4 cm diameter), the pterional transsylvian approach was used in 12 patients earlier in the series, and either the frontoorbito-zygomatic approach (seven patients) or the extended subfrontal approach incorporating a bilateral frontonasalorbital craniotomy (seven patients) was used later in the series. Following transcranial surgery there was one perioperative mortality secondary to a pulmonary embolism 2 months after surgery. The rate of CSF leak requiring lumbar drainage was 7.7% (two patients), and the rate of permanent visual worsening was 15.4% (four patients) after transcranial surgery.24 The rate of visual worsening was lower in the patients who underwent cranial base operations (7.8%); however, this was not statistically significant. Postoperative hypopituitarism occurred in six patients (23%), and permanent DI occurred in four patients (15%) after transcranial surgery. These complications were greater in the transcranial group compared with the transsphenoidal group. Only one patient (3.8%) in the transcranial group had complete tumor resection24 (Table 24.1).
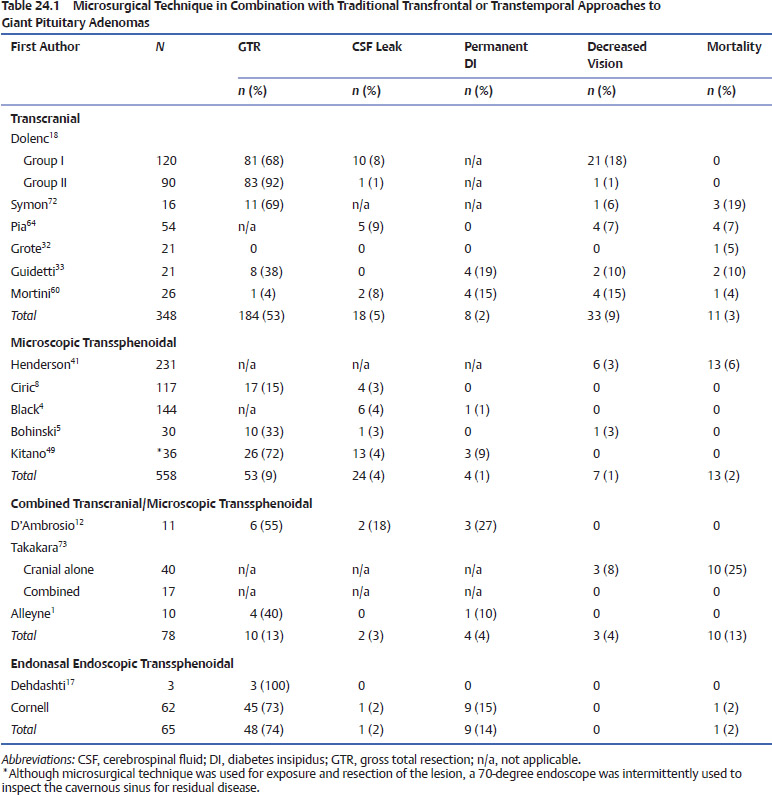
Other surgeons shifted to a combined transsphenoidal and pterional craniotomy approach to giant pituitary adenomas. In one series of 40 patients with giant pituitary adenomas (>5 cm in diameter) the older strategy of transcranial surgery alone was compared with a newer staged transsphenoidal and transcranial approach.7 In the older subgroup managed by transcranial surgery alone, a 25% mortality rate was reported, with the highest mortality rate, 57%, seen in the group who underwent radical surgical removal. This decreased to 26% in the partial-removal group. Worsening postoperative vision was noted in 10% after transcranial surgery, and the authors did not specifically report on endocrinologic outcomes7(Table 24.1). The high mortality rate led them to shift to an initial transsphenoidal removal of the intrasellar component of the tumor and decompression of the suprasellar component if it descends during the operation. The patients were then followed by repeat MRI scans for up to 3 months. At that time, suprasellar components descended into the vacant sella space and a second transsphenoidal or transcranial operation was performed. With this approach in 17 patients no operative mortality or major complications were reported; however, specific endocrine outcomes were not reported.7
The staged combined approach was also attempted as a simultaneous combined transsphenoidal and pterional approach.1,2 In a series of 10 patients who underwent the simultaneous combined surgical approach, six had gross total or near total removal of the tumor. All nine patients who presented with visual loss had postoperative resolution, and there was no operative mortality or postoperative CSF leak. Postoperative DI occurred in one patient, and hypopituitarism persisted in all five patients who presented with DI preoperatively1 (Table 24.1).
Improved visualization of the surgical anatomy with use of skull base techniques substantially decreased the operative morbidity and mortality of giant pituitary adenomas. In a series of 210 patients with large or giant pituitary adenomas with suprasellar and parasellar extension, a classic frontotemporal transcranial approach was used for the first 120 patients and an extradural transcavernous skull base approach was used for the next 90 patients.41 The skull base approach incorporated extradural anterior clinoidectomy, orbitotomy, optic canal unroofing, and intradural exposure of the cavernous sinus, and it combined intradural and extradural transcavernous tumor resection. Although the author’s exact definition of giant adenoma was unclear, these tumors required transcranial surgery for removal of their various suprasellar and parasellar extensions. With the classic approach in patients undergoing their first operation, complete resection was achieved in 63% of patients. New visual field deficits were observed in 29% of patients, and CSF leak occurred in 6% of patients. In contrast, with the extradural skull base approach, complete resection was achieved in 93% of patients. None of the patients who underwent the skull base approach had postoperative visual field deterioration or CSF leak.41 In both groups of patients, almost all had significant endocrinologic deficits present preoperatively, and they did not change after surgery. Specific anterior or posterior pituitary endocrine deficits were not reported. No perioperative mortalities were described with either approach (Table 24.1).
 Transsphenoidal Surgery for Giant Macroadenomas
Transsphenoidal Surgery for Giant Macroadenomas
The transsphenoidal approach for the resection of a pituitary tumor was first described by Herman Schloffer54 at the University Clinic in Innsbruck, Austria. He performed a superior nasal transsphenoidal approach on a 30-year-old man with a 6-year history of severe headaches and declining vision who was found to have an enlarged sella on a lateral skull x-ray. Although the surgery proceeded without serious complications, the patient died postoperatively from obstructive hydrocephalus. During the following years the transsphenoidal approach was modified, and Harvey Cushing was the first to present a large clinical series of 231 transsphenoidal pituitary adenoma resections in 1939.55 Cushing compared the clinical outcome between the transsphenoidal and transcranial approaches for resection of pituitary adenomas. In his series the perioperative mortality rate following transsphenoidal and transcranial pituitary adenoma resection was similarly low (5.2% versus 4.5%). However, the cause of death was different depending on the approach. Mortality following a transsphenoidal approach was due to infections, swelling of residual tumor tissue, and in one case uncontrollable intraoperative hemorrhage. Mortality following a transcranial pituitary adenoma resection was caused by postoperative blood clots in the majority of cases. Clinical follow-up data were available for almost all patients. Ten years after the operation half of the patients were still alive. Preoperative impaired vision improved in approximately two thirds of patients. Two major disadvantages of the transsphenoidal approach prompted Cushing to abandon the transsphenoidal approach. First, given the lack of preoperative imaging, possible suprasellar extension of a pituitary adenoma was unknown and the transsphenoidal approach was not suitable for intraoperative exploration. Consequently, tumor was left behind and caused half of the perioperative mortality associated with the transsphenoidal approach. Second, highpower illumination or magnification was not available, which severely limited access and visibility. Hence, in the late 1920s Cushing preferentially used the transfrontal approach, as it allowed for intraoperative visualization of suprasellar tumor extension and better decompression of the optic chiasm.
For the next decades the use of transsphenoidal operations diminished greatly. Two technologic milestones paved the way for the revival of the transsphenoidal technique. First, the intraoperative use of the operating microscope improved intraoperative illumination and visualization.56 Second, pre-operative CT provided information about the size and location of the lesion and facilitated patient selection and choice of appropriate surgical access. Using these technologic tools, a high incidence of complete tumor removal and low complication rate was reported for the transsphenoidal resection of pituitary microadenomas.57,58 Rapidly, transsphenoidal surgery was also adopted for pituitary macroadenomas.
In 1983, Ciric and colleagues59 reported transsphenoidal resection of pituitary macroadenomas (diameter >2 cm) in 108 patients. No perioperative mortality was encountered. Preoperative visual field impairment improved in 90% of patients. Normalization of prolactin- and GH-secreting tumors was achieved in approximately one third of the patients. Specific anterior or posterior pituitary endocrine deficits were not reported, and no case with DI lasting longer than 3 months was seen. Postoperative CT imaging revealed gross total tumor resection in 59% of patients; however, this number might be optimistic, given that CT imaging was used. The main complication in this series was CSF rhinorrhea, which complicated the postoperative course of 3.5% of patients, and one of these patients developed meningitis (Table 24.1).
Black and colleagues60 described their experience with transsphenoidal procedures for pituitary adenomas in 255 patients. Of these lesions, 44% had suprasellar extension and 15% were intrasellar macroadenomas. In this series there was no perioperative death. Importantly, Black and colleagues correlated complications with tumor size. CSF leaks were the major complication encountered. Although only 1% of microadenomas were complicated by CSF leaks, this complication was seen in 3% of tumors with suprasellar extension and 9.5% of macroadenomas (>1 cm in diameter). A similar increase of adverse outcome was seen with regard to the rate of DI following removal of microadendomas (1%) and macroadenomas (9.5%). In all but one patient (0.4%), DI resolved within 1 year (Table 24.1). This study was limited to perioperative complications and did not address the radiographic extent of resection and clinical outcome.
Bohinski and colleagues61 used intraoperative MRI to study the extent of resection in 30 patients who underwent transsphenoidal resection of pituitary macroadenomas (measuring ≥1 cm). In this series, a gross total resection was achieved in 34% of patients (Table 24.1). One transsphenoidal approach was converted to a craniotomy due to laceration of the anterior cerebral artery.
Han and colleagues62
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


