Excision of Tumors of the Prestyloid Parapharyngeal Space
Excision of Tumors of the Prestyloid Parapharyngeal Space
Kerry D. Olsen
INTRODUCTION
Tumors of the prestyloid parapharyngeal space are uncommon but challenging due to the variety of lesions encountered and the complex anatomy of the involved area. Fortunately, these tumors are generally benign, and therefore, they bring expectations from the patient and the physician that excision should lead to low morbidity and very low mortality. Since patients rarely die of these tumors, the goal of management should be to perform the operation safely with complete removal of the tumors to minimize the risk of recurrence and to preserve surrounding structures.
The prestyloid portion of the parapharyngeal space is actually a potential space. It contains adipose tissue, a portion of the deep lobe of the parotid gland (the retromandibular portion), minor salivary glands, and scattered vessels and nerves (Table 29.1). Tumors of salivary gland origin in the pharyngeal space have the same distribution as those in the parotid gland, that is, 80% to 90% are benign and 10% to 20% are malignant. The majority are pleomorphic adenomas. The challenge to the surgeon is understanding tumor behavior and appropriate preparation to manage the simple and complex tumors that are encountered in this area.
It is essential that the surgeon is familiar with the anatomy. The prestyloid space superiorly is contained by fascial areas that direct tumor growth. The parapharyngeal space itself is divided into the pre- and poststyloid areas by the fascia of the styloid process that connects to the tensor veli palatini muscles and its surrounding fascia (Fig. 29.1). Another important structure is the stylomandibular ligament that forms part of the boundary of the stylomandibular tunnel. The stylomandibular ligament unites the fascia of the styloid process to the angle of the mandible. It can be thinned by tumors but is always present, and its division insures adequate opening of the parapharyngeal space and successful subsequent tumor removal. It is also a structure where constriction can occur as tumors grow between the mandible and this ligament. This leads to the classic “dumbbell” tumors that extend from the tail of the parotid gland into the parapharyngeal space. Table 29.2 lists the anatomic boundaries of the prestyloid space.
HISTORY
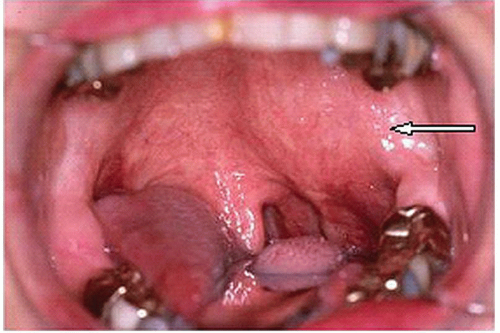
Most tumors of the prestyloid space are benign and, as such, have a slow growth rate and generally are asymptomatic. The majority are discovered on routine physical examination when a physician, or the patient, notices a bulging or displacement of the nonrigid portions of the parapharynx: generally the medial surface, the displacement of the constrictor muscles, or the inferior soft border near the inferior aspect of the parotid gland or digastric muscle. For prestyloid tumors, displacement of the lateral pharyngeal wall usually occurs in the region of the tonsil or soft palate or anterior tonsillar pillar (Fig. 29.2). Eventually, as the tumors enlarge, they will displace the entire tonsil and lateral pharynx up to the nasopharynx. One may notice tumors in the deep lobe of the parotid that also extend through the stylomandibular tunnel and present as a swelling or mass in the pretragal area, as well as the pharynx. It is common today to discover prestyloid lesions on routine imaging—CT or MRI scans—done for other indications.
TABLE 29.1 Structures Contributing to Tumors of the Prestyloid Parapharyngeal Space
Adipose Tissue
Deep lobe of the parotid gland
Minor salivary glands and ectopic salivary rests
Muscles
Nerves
Vessels
As these tumors extend superiorly, the muscles of the eustachian tube can be compressed, causing a feeling of fullness and pressure in the ear. Eustachian tube dysfunction can also lead to middle ear effusion with decreased hearing. Involvement of the medial pterygoid muscle can lead to trismus, which is more common with malignant tumors. As the tumor enlarges, it displaces the pharynx and interferes with eating, speech, and especially sleep. Some of the early symptoms are snoring or symptoms of obstructive sleep apnea. This occurs before these tumors impact eating and phonation.
There are several cases of prestyloid parapharyngeal lesions that were untreated in elderly sick individuals that enlarged to the point where they caused significant dysphagia, inanition, respiratory distress, and death. It is also not uncommon for lesions of the prestyloid parapharyngeal space to be confused with pathology of the tonsil, such as infection, enlargement, or tumors. Pain is not a common finding, but if it is present, one must be concerned about a malignant lesion. Other symptoms of malignancy, of course, include the presence of facial nerve involvement and regional adenopathy.
PHYSICAL EXAMINATION
Small tumors, due to their location in the prestyloid parapharyngeal space, cannot be detected on physical examination. A tumor must be >3 cm to cause displacement of the surrounding structures before it can be seen or felt. Early tumors are detected only serendipitously on a prior imaging study. It is important to carefully inspect the pharynx and the parotid gland and palpate both intraorally and bimanually. A palpable deep parotid mass that is immobile and of indeterminate deep extent may extend into the parapharyngeal space. One must assess the function of the seventh cranial nerve and palpate the parotid and neck carefully for any enlarged nodes. In a series from Mayo Clinic of almost 200 parapharyngeal tumors, an intraoral mass alone occurred in 63%, an external mass in the parotid region was present in 58%, and both findings were found in only 28% of the cases.
FIGURE 29.1 Division of the parapharyngeal space into prestyloid and poststyloid compartments.
TABLE 29.2 Anatomic Boundaries of the Prestyloid Parapharyngeal Space
Superior
Fascial junction of the medial pterygoid and tensor veli palatini fascia
Superior medial
Fascia from the tensor veli palatini muscle to the spine of the sphenoid
Medial
Superior constrictor muscles
Inferior medial
Fascia of the constrictor muscles joins the fascia of the styloglossus and stylopharyngeus muscles
Superior lateral
Fascia of the medial pterygoid muscles and ramus of the mandible
Lateral
Retromandibular portion of the deep lobe of the parotid gland
Inferior lateral
Fascia extension that forms the stylomandibular ligament
Inferior
Posterior belly of the digastric muscle
INDICATIONS
Parapharyngeal deep lobe benign parotid tumors
Parapharyngeal deep lobe malignant parotid tumors
Mesenchymal tumors located in the prestyloid space
CONTRAINDICATIONS
As with any mass of the parotid gland, the decision to operate must take into consideration the patient’s age, the patient’s health, his or her wishes, and the surgeon’s experience. In addition, one should have available key colleagues, including pathologists, to complete the procedure as dictated by the pathologic findings.
The final recommendation for surgery is always individualized based upon the patient, the history, the examination, and the evaluation. The discussion about removing a benign pleomorphic adenoma from the parapharyngeal space is vastly different than that of an obvious malignant tumor in this region.
PREOPERATIVE PLANNING
Management of a prestyloid parapharyngeal tumor is approached similar to any mass discovered in the parotid gland on physical examination. Whether it is felt on clinical examination or noted on imaging studies, the evaluation is the same. Since prestyloid tumors are usually of salivary gland origin, awareness of a mass will lead to a recommendation for removal—for diagnosis, to prevent growth, and to prevent malignant degeneration.
FIGURE 29.2 Typical displacement of the anterior tonsil region from a mass in the parapharyngeal space (arrow).
TABLE 29.3 Tumors of the Prestyloid Parapharyngeal Space
Benign
Malignant
Pleomorphic adenoma
Warthin tumor
Oncocytoma
Benign lymphoepithelial lesion
Hemangioma
Branchial cleft cyst
Venous malformation
Fibroma
Schwannoma
Neurofibroma
Rhabdomyoma
Hibernoma
Mucoepidermoid carcinoma
Adenocarcinoma
Acinic cell carcinoma
Adenoid cystic carcinoma
Carcinoma ex pleomorphic adenoma
Hemangiopericytomas
Variety of sarcomas
Only gold members can continue reading. Log In or Register to continue