Masses arising in the buccal space or in the accessory lobe of the parotid gland are uncommon and may present as a visible mass in the cheek or as a mass distorting the buccal mucosa. Since a wide variety of tumors arise in this area, a precise diagnosis is often difficult to make. A detailed history, clinical examination, and imaging studies are essential in defining the location and extent of these tumors. Although fine-needle aspiration biopsy (FNAB) may provide important diagnostic information, only complete excision of the mass with histopathologic evaluation will provide a definitive diagnosis.
Most of the tumors in the buccal space are benign and are of salivary gland origin. However, other types of benign as well as malignant tumors and other histologic types may arise in this area. Rarely, cancer metastatic from a distant site will present a challenge in diagnosis and management. Table 30.1 lists the lesions from our own experience and those reported in the literature. The operative techniques for removal of these tumors are challenging because the technique must provide good exposure for tumor removal in order to prevent damage to the facial nerve and Stensens duct and to assure a good cosmetic outcome.
HISTORY
The finding of a mass within the substance of the cheek poses a diagnostic problem since this may arise from many types of tissues present in the buccal space or may be metastatic from a distant site. A detailed history, clinical examination, and imaging studies are important in arriving at a specific diagnosis. However, the final diagnosis is often elusive and must be confirmed by surgical excision and histopathologic evaluation. Obviously, pain, infiltration of the overlying facial skin, and facial weakness suggest malignancy.
A mass in the buccal space presents in a unique fashion. These are readily apparent because they may be seen just deep to the skin of the cheek or in the buccal mucosa. The typical history encountered in such patients is that of a slowly growing, painless mass in the cheek, which disturbs facial symmetry. The mass is usually nontender and rarely is pain or facial nerve paralysis noted at the time of presentation. The mass may lie closer to the buccal mucosa so that the patient may discover the intraoral mass by feeling it with their tongue. In some patients, the mass interferes with their dentures fitting properly.
PHYSICAL EXAMINATION
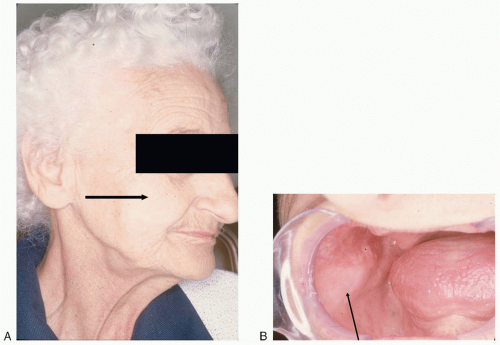
A mass in the buccal space, which presents externally, should be inspected carefully, and the dimensions of the lesion should be measured and recorded. These lesions are typically nontender and should be evaluated by bimanual palpation. Stensens duct should be identified and an attempt should be made to express saliva from the duct. Detailed inspection of facial nerve function must be carried out. Any sign of weakness of the facial nerve should be recorded since this will have an impact on the plan for surgical management. Fixation of the skin, obstruction of Stensens duct, facial weakness, and pain are suggestive of a malignant tumor. In some instances, particularly in very thin individuals, the mass may be visible both externally and internally (Fig. 30.1).
TABLE 30.1 Lesions Reported in the Buccal Space
Glandular
Vascular
Lymph Node
Connective
Muscular
Inflammatory
Neural
Miscellanous
Accessory parotid or aberrant salivary gland tumors
False Aneurysm
Benign reactive lymph node
Alveolar soft part sarcoma
Masseteric hypertrophy
Abscess
Neurofibroma
Clear cell carcinoma metastatic from kidney
Acinic cell carcinoma
Hemangioma
Calcified lymph node
Fibroma
Myositis ossificans
Aspergilloma
Neuroma
Foreign body granuloma, for example, paraffinoma
Adenoid cystic carcinoma
Hyalinized thrombus
Lymphangioma
Fibromatosis
Polymorphous low-grade adenocarcinoma
Kimura disease
Carcinoma ex pleomorphic adenoma
Recurrent juvenile nasopharyngeal angiofibroma
Lymphoma
Fibrosarcoma
Sarcoidosis
Chronic sialadenitis
Lymphosarcoma
Lipoma
Tuberculous granuloma and adenoid cystic carcinoma presenting as a single mass in the buccal space
Minor salivary gland calculus
Metastatic lymph node involvement
Liposarcoma
Mixed tumors (benign and malignant)
Nodular fasciitis
Masseteric hypertrophy
Mucoepidermoid carcinoma (low- and high-grade
Pseudoherniation of buccal fat pad
Oncocytoma
Rhabdomysarcoma
Papillary cystadenoma lymphomatosum
Solitary fibrous tumor
Parotid duct tumor or calculus
Spindle cell lipoma
Sebaceous adenoma
FIGURE 30.1 A: External view of a mass in the right buccal space mass. B: Note the intraoral bulge produced by the mass.
Only gold members can continue reading. Log In or Register to continue