The modern rhinologist has a wide variety of powered tools at his or her disposal. Innovations in powered instrumentation include the suction-irrigation drill, the coblator, and the introduction of a bone-cutting ultrasonic aspirator. The primary drawback of powered instruments continues to be the higher costs associated with their use, whereas their main advantage is the ability to accomplish multiple functions, such as bone removal, suction, and irrigation, with one tool. The effective use of any powered instrument requires an intimate understanding of its capabilities and limitations. This article provides a brief review of powered instrumentation used in endoscopic sinus and skull base surgery and explores the history, technical details, and potential applications of these exciting tools. Evolution in the design and functioning of the microdebrider are discussed elsewhere.
The introduction of the rigid nasal endoscope for the diagnosis and surgical management of sinonasal disorders is the single greatest advance in rhinology to date. Endoscopy provided improved visualization of sinonasal anatomy and pioneered the way for sinus surgery to safely extend beyond the nasal cavity and paranasal sinuses. However, with one hand occupied holding the endoscope, the surgeon is left with only one free hand with which to operate. A logical development from this reality is a need for surgical instruments that could perform a variety of tasks at once. In addition, the desire of endoscopic surgeons to access different regions of the adjacent intracranial cavity and orbit necessitated the development of tools that permitted the safe removal of significant amounts of bone in a controlled and expeditious manner.
Powered sinus instruments entered the landscape several decades ago, with the introduction of the microdebrider. Since then, several other powered tools, such as the endoscopic drill (equipped with suction-irrigation), coblator, and the ultrasonic aspirator have been used during endoscopic sinus and skull base surgery. As with the microdebrider, these innovations may also one day become a mainstay of the rhinologist’s arsenal. The primary drawback of powered instruments over conventional tools continues to be the higher costs associated with their use, which include the initial capital expenditure for the system and ongoing costs of disposable blades, bits, tips, and tubing. It should be noted that the effective use of powered instrumentation requires an intimate understanding of the capabilities and limitations of these instruments. In contradistinction to conventional instrumentation, powered tools, by definition, have an electrical supply enabling them to move very rapidly and are often equipped with continuous suction. This has raised concerns over the potential for the rapid escalation of complications, if and when they occur. It should be underscored, however, that these are still tools nonetheless, and they are not in and of themselves more or less dangerous, provided the operator possesses the requisite surgical experience and understanding of both the disease process and the tools selected to modify it.
Endoscopic drills
Endoscopic drills are far less commonly used than the microdebrider, given that the microdebrider is able to effectively handle the thin bony partitions of the ethmoid that are addressed with most endoscopic sinus procedures. Where the bone is thicker than microdebrider blades can handle, a variety of drills and drill bits have been developed for endoscopic use. Conventional instruments can sometimes be used in cases requiring significant bony removal, but the greater force needed to take down thick bone can result in poorly controlled movements that risk injury. The advantage of drills in this setting is that they permit expeditious and more controlled bony removal.
Technology
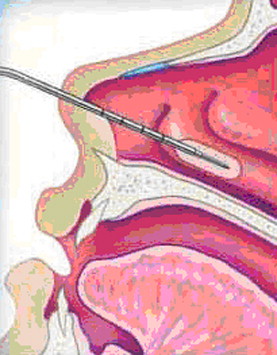
Unlike the more familiar otologic drills, drills intended for endoscopic use ideally have a slimmer profile permitting them to be passed readily into and out of the nostrils. They also often have a protective sheath that protects tissues from the posterior aspect of the drill burr and are equipped with continuous suction and irrigation functions ( Fig. 1 ). A significant drawback to the sheaths, however, is that they do increase the diameter of the drill and thus contribute to decreased visualization of the already narrow surgical field. The advantages and disadvantages of the guarded drills must be reconciled depending on the details of the case and the anatomic configuration encountered.

With all drills, the number of flutes on the burr determines how aggressively the drill will function. Fewer flutes will result in faster and more aggressive takedown of bone, but often at the expense of control. Increasing the speed of rotation also provides more rapid removal of bone, although in this case there is actually improved control with a faster spinning burr. Diamond burrs are much less aggressive than cutting burrs in general and are available for smoothing bone edges, although these tend to be much slower at takedown of bone than cutting burrs. This makes them the better choice where a longer operative time is a worthwhile price to pay to minimize risks of damage to delicate surrounding structures. Endoscopic drills also have built-in suction to constantly remove blood and debris and thus allow for improved visibility. This is a very valuable feature.
Clinical Applications
Drills are not needed for routine endoscopic sinus surgery. However, they can be very beneficial for more advanced techniques that require the removal of thicker bone. A variety of clinical scenarios and procedures may be augmented with the use of high-speed drills. Perhaps the most common application of drills is in surgery of the frontal sinus. After conservative measures aimed at widening the frontal recess fail, more aggressive techniques targeting the frontal sinus ostium and the floor of the sinus are pursued. The frontal ostium is located in the posteromedial aspect of the thick floor and can be enlarged unilaterally or bilaterally using a drill. The high-speed drill is effective at resecting the floor and nasofrontal beak region and maybe used to create a large common aperture that drains both frontal sinuses via the endoscopic modified Lothrop procedure (EMLP; also known as the Draf III or bilateral frontal drillout procedure) ( Fig. 2 ). This technique was described by Draf and others and involves resection of both frontal sinus floors and interfrontal septum through a superior septectomy. A meta-analysis of the EMLP demonstrated that in experienced hands, this technique is very effective in the management of refractory frontal sinus disease and is associated with a low rate of complications (<1% major and 4% minor complication rates). During this procedure, drilling proceeds from the frontal ostium anteriorly through the frontal floor and nasofrontal beak area, and great care must be taken to avoid trauma to the skull base and anterior ethmoidal artery, which constitute the posterior boundary of the dissection. The burr guard available on some endoscopic drills may be of considerable value when drilling out the frontal sinus, where damage to the posterior aspect of the ostium and recess can lead to unwanted mucosal trauma and resultant stenosis or possibly even intracranial injury.
The proliferation of endoscopic transsphenoidal approaches to the sella and beyond have created novel clinical situations that require the controlled removal of bone from virtually all aspects of the sphenoid sinus, beginning at the face for initial access, through the posterior and superior walls toward the clivus and sellar regions, and laterally for decompression of the optic nerve. Suction-irrigation drills are important during these procedures not only to continuously evacuate blood and debris from the field to maximize visualization but also to limit the transmission of heat to adjacent vital structures such as the optic apparatus and brain.
Drills have also influenced endosopic surgery of the orbit and lacrimal system. Endoscopic orbital techniques offer the advantages of enhanced visualization and more direct access to the posterior orbit and apex while also avoiding any facial scars. Performing a successful endoscopic dacryocystorhinostomy (E-DCR) for nasolacrimal duct obstruction requires the creation of a generous bony rhinostomy through, in part, the thick ascending process of the maxilla, with bone removal beginning in the region of the maxillary line and proceeding anteriorly. Although many techniques for bone removal have been described, including the use of a mallet and osteotome, microdebriders, and lasers, many surgeons prefer the finesse and precision best afforded by a high-speed drill. Removal of thick bone during orbital decompression (for lateral and inferior walls especially) and optic nerve decompressions may also be augmented by the use of a drill.
The bone of the maxilla can also be removed posteriorly with a drill for exposure of the pterygopalatine fossa, as part of the endoscopic transpterygoid approach to the lateral recess of the sphenoid sinus. Drills have also been applied for the transnasal resection of sinonasal fibro-osseous lesions and large septal spurs during septoplasty. The use of a drill is also recommended to superficially shave the underlying bone in cases of inverted papilloma to eliminate any small foci of tumor at the site of attachment. Even where the attachment is along the thin lamina papyracea, a diamond burr can be used to gain an added element of control after gross tumor has been removed.
Coblation
Technology
Coblation is a relatively new technology that was patented by ArthroCare (Austin, TX) in 1997, initially intended for cartilage ablation during arthroscopy. The Food and Drug Administration approved this technology for use in otolaryngology in 2000. It uses radiofrequency energy to energize electrolytes within a conductive medium (typically saline). This theoretically creates a plasma field that disrupts molecular bonds within the surrounding tissues at relatively low temperatures (40°C–70°C as compared with more than 400°C with monopolar electrocautery). Because some studies suggest that a plasma field is unlikely to be created outside a vacuum, Zinder theorized that the decreased thermal damage during coblation has more to do with vaporization of the saline solution than creation of a plasma field. In any event, there indeed does appear to be significantly less penetration of thermal energy into the surrounding tissue with the use of this technology, which may be advantageous.
Clinical Applications
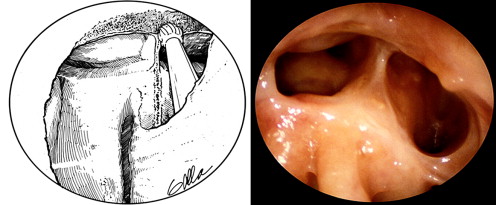
The most common use of coblation in otolaryngology at the present time is during tonsillectomy, where some studies have suggested less postoperative pain and a faster recovery. However, coblation is rapidly gaining popularity in rhinologic surgery for inferior turbinate reduction. Separate wands are available for adult and pediatric patients. Coblation is performed at several marked depths to create a series of ablated pockets submucosally within the erectile tissue of the inferior turbinate, which provides immediate volume reduction and will further scar down during healing ( Fig. 3 ). Back and colleagues showed significant subjective improvement in nasal obstruction, sneezing, crusting, and nasal discharge using a visual analog scale after coblation-mediated inferior turbinate reduction. There is a paucity of well-designed randomized studies directly comparing coblation to other methods of turbinate reduction, but current literature does suggest promising short-term and even long-term results with this technique. Coblation has also been proposed for use in nasal polypectomy and transnasal tumor resection, where its hemostatic ability could provide essentially bloodless removal of soft tissue. However, there is little in the literature at the present time on this application. A major limitation to the use of currently available coblation technology to endoscopic sinus surgery for chronic sinusitis with or without nasal polyps is its inability to address the bony partitions encountered in the ethmoid sinus.