35
Evaluation and Management of Pulsatile Tinnitus
Aristides Sismanis
Pulsatile tinnitus (PT) is an uncommon type of tinnitus which often presents a diagnostic and management dilemma to the clinician. Correct diagnosis is essential because many patients with this symptom have a treatable underlying cause. Furthermore, failure to establish the appropriate diagnosis may have disastrous consequences because in some patients an associated life-threatening pathology may be present.
 Pathophysiology and Classification
Pathophysiology and Classification
PT most often originates from vascular structures within the cranial cavity, head and neck region, or even the thoracic cavity, and is transmitted to the cochlea by bony or vascular structures. PT arises either from increased flow volume or stenosis of a vascular lumen and according to the vessel of origin it can be classified as arterial or venous. The venous type can originate not only from primary venous pathologies, but also from conditions causing increased intracranial pressure (ICP) by transmission of arterial pulsations to the dural venous sinuses.1 In rare instances, PT originates from other nonarterial structures and is classified as nonvascular.
PT is classified as objective if it is audible to both the patient and examiner, or as subjective if it is audible only to the patient.
High-pitched tinnitus, often bilateral, with a pulsatile component should not be confused with arterial PT. This type of tinnitus is usually associated with high-frequency sensorineural hearing loss and is subjective (See Chapter 36).
 Arterial Etiologies
Arterial Etiologies
Atherosclerotic Carotid Artery Disease
In our experience atherosclerotic carotid artery disease (ACAD) has been the most common cause of PT in patients older than 50 years, especially when associated risk factors such as hypertension, angina, hyperlipidemia, diabetes mellitus, and smoking are present. Objective PT can be the first manifestation of ACAD in some of these patients.2 PT in ACAD is secondary to bruit(s) produced by turbulent blood flow at stenotic segment(s) of the carotid artery. In a series of 12 patients with PT secondary to ACAD, ipsilateral carotid bruit was present in all of them. Atherosclerotic subclavian artery disease and atherosclerotic occlusion of the contralateral common carotid artery also have been reported in association with PT.3,4 Diagnosis is confirmed by duplex ultrasound studies.2
Vascular Neoplasms of Skull Base and Temporal Bone
Glomus jugulare and tympanicum are the most common vascular tumors of the temporal bone presenting with PT.5 Other rare middle ear neoplasms associated with PT include hemangiomas,6 angiomatous meningiomas,7 and metastatic breast carcinomas.8
Intracranial Vascular Abnormalities
Intracranial vascular abnormalities are uncommon etiologies of PT; however, misdiagnosis may lead to catastrophic consequences for patients. At our institution the most common vascular intracranial abnormality presenting with PT is dural arteriovenous fistula (AVF).
Dural AVFs comprise approximately 15% of intracranial arteriovenous malformations (AVMs) and usually become symptomatic during the fifth or sixth decades of life.9,10 PT is the most common manifestation of these lesions. The transverse and sigmoid dural sinuses are most commonly involved, followed by the cavernous sinus. In contrast to AVMs, AVFs are usually acquired and thought to result from spontaneous dural venous sinus thrombosis, or secondary to trauma, obstructing neoplasm, surgery, or infection. As the thrombosed segment recanalizes, ingrowth of dural arteries takes place and arterial-to-sinus anastomoses are formed.9
Pulsatile tinnitus in these patients is of the arterial type and is associated with a bruit over the involved dural sinus (usually audible in the retroauricular area) as well as objective PT (audible in the ear canal). Fig. 35–1 depicts a carotid angiogram of a patient with an AVF between a posterior meningeal branch of the middle meningeal artery and the transverse sinus.

Figure 35–1 Carotid angiography, lateral projection. An arteriovenous fistula (AVF) is shown (arrow) between a posterior meningeal branch of the middle meningeal artery and the transverse sinus.
The mortality rate from hemorrhage of dural AVFs has been reported to be between 10 and 20%.9 In cases with retrograde drainage into the cortical veins, the chance of subarachnoid or parenchymal hemorrhage is much higher.9
Dissecting aneurysms are also rare, and more often involve the internal carotid arteries and less often the vertebral arteries.11 Besides objective PT and cervical bruit, manifestations include cervical pain, headache, cerebral ischemic symptoms, cranial neuropathies, vertigo, dysgeusia, and Horner’s syndrome.9,11 The most common angiographic finding is that of irregular stenosis.11
Sudden head rotation, especially when accompanied by extension (i.e., the tennis “ace serve”), is a common precipitating event.12 Fibromuscular dysplasia (FMD) and various arteriopathies such as Marfan syndrome can be predisposing factors.13 Aneurysms of the intrapetrous carotid artery,14–16 and of the anterior communicating artery17 are very rare causes of PT.
Fibromuscular Dysplasia
Fibromuscular dysplasia is a nonatherosclerotic, noninflammatory stenosing vascular disease, which affects younger females and most commonly involves the renal and internal carotid arteries.18
Carotid artery FMD is frequently associated with PT. Other symptoms such as vertigo, headache, cervicofacial hypoesthesia, and transient ischemic attacks have been reported.19 20 The typical angiographic finding is that of a “string of beads.”20 The prevalence of intracranial aneurysms in these patients is approximately 7%.21 Fig. 35–2 is a carotid angiogram of a 36-year old woman with FMD.
Tortuous Carotid Artery
These are usually middle-aged patients with audible bruits in the skull base. Diagnosis can be made with computed tomography (CT) angiography. It is likely that aging results in tortuous carotid vessels with associated turbulent blood flow and PT. In our experience PT subsides spontaneously with time in most of these cases. Table 35–1 summarizes the less common arterial etiologies of PT.5,22–36
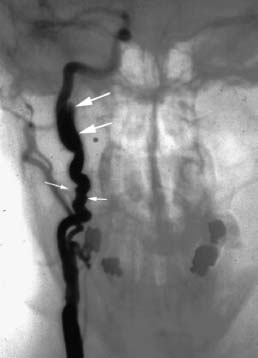
Figure 35–2 Carotid angiography, anterior-posterior view, of a 36-year-old woman with fibromuscular dysplasia. The “string of beads” is a pathognomonic finding (arrows).
 Venous Etiologies
Venous Etiologies
Idiopathic Intracranial Hypertension Syndrome
Idiopathic intracranial hypertension (IIH) syndrome is a common cause of venous PT in obese female patients. This syndrome is of unknown etiology in most cases, and is characterized by increased intracranial pressure, normal cerebrospinal fluid (CSF) content, and absent neurologic signs except for occasional V, VI, and VII cranial nerve palsies.37,38 Other synonyms of this disorder are pseudotumor cerebri and benign intracranial hypertension syndrome; the latter term is recently used less often because the risk of visual loss is not “benign.” Etiologies of this entity are summarized in Table 35–2.38–42
| Intrapetrous carotid artery dissection34 |
| Brachiocephalic artery stenosis23 |
| External carotid artery stenosis27 |
| Ectopic intratympanic carotid artery22,29,35 |
| Persistent stapedial artery32 |
| Aberrant artery in the stria vascularis30 |
| Vascular compression of the eighth nerve31 |
| Increased cardiac output (anemia, thyrotoxicosis, pregnancy)24,25 |
| Paget’s disease26,28,33 |
| Aortic murmurs36 |
| Otosclerosis5 |
| Hypertension; antihypertensive agents5 |
The annual incidence of IIH hypertension is 0.9 per 100,000 people in the general population. This entity is more common in young African-American females who are 20% percent or more above their ideal body weight.1,43,44 In males this disorder is very rare, and in 25% of patients it may become chronic.37
Although the classic presentation of IIH consists of headaches or visual disturbances, PT alone or in association with hearing loss, dizziness, and aural fullness has been reported as the main manifestation(s) of this syndrome.45–47 Many of these patients are morbidly obese (body weight more than 100 lbs above ideal weight) and have associated papilledema. Absence of papilledema. however. does not exclude this entity.48–50
Significant uncertainty exists regarding the pathophysiology of IIH. Many studies have tried to elucidate the underlying cause. often with conflicting results. Proposed theories include increased CSF production. cerebral edema. decreased CSF absorption. and elevated cerebral venous pressure.38,39,43,51,52 The pathophysiology of IIH in morbidly obese patients most likely results from increased intraabdominal and intrathoracic pressure. cardiac filling. and intracranial venous pressures.53 This pathophysiologic mechanism is further supported by an animal study demonstrating increased CSF pressure when intraabdominal pressure was acutely raised.54 Increased cerebral blood flow secondary to cerebrovascular resistance changes and CSF hypersecretion induced by elevated estrogen levels also have been reported as pathophysiologic mechanisms of IIH.55
| Medications |
| Amiodarone |
| Anabolic steroids |
| Chlordecone |
| Corticosteroids |
| Cyclosporine |
| Diphenylhydantoin |
| Divalproate |
| Growth hormone |
| Indomethacin |
| Leuprorelin acetate |
| Levothyroxine |
| Lithium carbonate |
| Minocycline |
| Nalidixic acid |
| Norplant |
| Penicillin |
| Sulfa antibiotics |
| Tetracyclines and related compounds |
| Vitamin A |
| All-trans-retinoic acid |
| Endocrine Disorders |
| Adrenal insufficiency |
| Hypoparathyroidism |
| Hyperthyroidism |
| Obesity |
| Menarche |
| Menstrual irregularities |
| Pregnancy |
| Polycystic ovary syndrome |
| Nutritional Disorders |
| Hypervitaminosis A |
| Hypovitaminosis A |
| Hyperalimentation in nutritional deficiency |
| Obstruction to Venous Drainage |
| Cerebral venous thrombosis |
| Hypercoagulable states |
| Antiphospholipid antibody syndrome |
| Polycythemia |
| Mastoiditis |
| Superior vena cava syndrome |
| Increased right heart pressure |
| Bilateral radical neck dissection |
| Circulatory and Hematologic |
| Iron-deficiency anemia |
| Sickle cell anemia |
| Pernicious anemia |
| Gastrointestinal hemorrhage |
| Cryofibrinogenemia |
| Systemic Disorders |
| Lupus erythematosus |
| Sickle cell anemia |
| Sarcoidosis |
| Sleep apnea |
| Turner’s syndrome |
| Human immunodeficiency virus infection |
| Paget’s disease |
| Galactosemia |
| Head trauma |
| Nephrotic syndrome |
| Uremia |
| Infectious |
| Lyme Disease |
| Infectious mononucleosis |
PT in IIH syndrome results from the systolic pulsations of the CSF. which originate mainly from the arteries of the circle of Willis. These pulsations. which are increased in magnitude in the presence of intracranial hypertension. are transmitted to the exposed medial aspect of the dural venous sinuses (transverse and sigmoid) and compress their walls synchronously with the arterial pulsations.1,56 The resulting periodic lumen narrowing converts the normal laminar blood flow to turbulent. thus producing a low-frequency PT.1 The low-frequency sensorineural hearing loss seen in many of these patients is believed to result from the masking effect of the PT. This is supported by the fact that light digital compression over the ipsilateral internal jugular vein (IJV) results in cessation of the tinnitus and immediate improvement or normalization of hearing.1 Stretching or compression of the cochlear nerve and brainstem. caused by the intracranial hypertension or possible edema. may also play a role in the hearing loss and dizziness encountered in these patients. This is supported by the abnormal auditory brainstem response (ABR) present in one third of these patients.57
Magnetic resonance venography (MRV) can be very helpful in identifying cerebral venous thrombosis and has been recommended for IIH patients.58,59 In a recent study. autotriggered elliptic-centric-ordered (ATECO) three-dimensional gadolinium-enhanced MRV identified bilateral sinovenous stenosis in 27 of 29 patients with IIH and only in 4 of 59 controls. It was not clear whether the stenosis was a cause or effect of intracranial hypertension.60 Anatomic obstruction of the venous transverse sinuses has recently been reported in IIH patients. and direct retrograde cerebral venography (DRCV) with manometry has been recommended to establish the diagnosis.61.62
Diagnosis is made by exclusion of other causes of intracranial hypertension and is established by lumbar puncture with confirmation of CSF pressure of more than 200 mm of water with normal CSF constituents.
Jugular Bulb Abnormalities
High-placed and dehiscent jugular bulbs are the most common reported jugular bulb abnormalities.63–66 Fig. 35–3 shows a CT angiogram of a patient with an enlarged dehiscent jugular bulb and an associated diverticulum. A bluish and inferiorly based retrotympanic lesion is the typical otoscopic finding.
Idiopathic or Essential Pulsatile Tinnitus
Idiopathic or essential PT and venous hum are terms used interchangeably in the literature to describe patients with PT of unclear etiology.67.68 The most common age group of patients with idiopathic PT is between 20 and 40 years and there is a marked female preponderance.1 A possible cause of idiopathic PT is believed to be turbulent blood flow produced in the IJV as it curves around the lateral process of the atlas.69
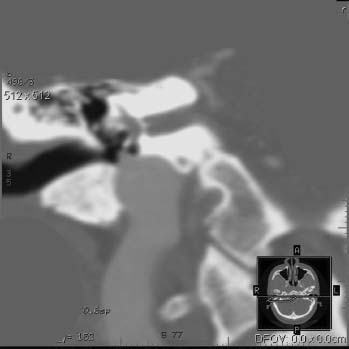
Figure 35–3 Coronal computed tomography (CT) angiogram, venous phase, shows an enlarged dehiscent jugular bulb with an associated diverticulum.
Diagnosis of this condition should be made only after appropriate evaluation and elimination of other disorders, such as IIH syndrome. Because it is possible that many of the patients reported in the literature with idiopathic PT had an incomplete evaluation to rule out IIH syndrome, it is possible that at least in some of these cases, PT was secondary to this syndrome. Associated symptoms of headaches and blurred vision, especially in morbidly obese female patients, should alert the physician to IIH syndrome. Table 35–3 summarizes the venous etiologies of PT.1,63–73
 Nonvascular Etiologies
Nonvascular Etiologies
Palatal, Stapedial, and Tensor Tympani Muscle Myoclonus
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


