24 European Position Paper on Rhinosinusitis and Nasal Polyps • Rhinosinusitis: – Facial pain/pressure – Hyposmia/anosmia – Mild = 0 to 3 – Moderate = >3 to 7 – Severe = >7 to 10 • Epidemiology: – 8.4% of Dutch population suffer with ≥ 1 episode of ARS/year – Fifth most common reason for ABx prescription in the United States – 11% of population suffer with CRS (prevalence) – ≥15% of outpatient consultations in ENT – 10,000 sinus procedures per year in the United Kingdom (1999–2010) – Cost of $500 per year to patients with CRS in the United States – Increasing incidence of CRS with increasing age—mean age of 53 – Slight male preponderance – AFRS accounts for ~10% of CRS with nasal polyps (CRSwNPs) • Bacterial superinfection of virally damaged mucosa: – Streptococcus pneumoniae – Haemophilus influenzae – Moraxella catarrhalis (esp. children) • Ciliary impairment—impaired by viral infection • Allergy—may be a factor but evidence limited • Helicobacter pylori and laryngopharyngeal reflux (LPR)—little evidence • Presence of NG tube • Ciliary impairment—secondary ciliary dyskinesia • Allergy—may be present in 50 to 90% of patients • Asthma—many asthmatics will show abnormal mucosal CT findings (approximately 88%) • Immunocompromised state—low IgA, IgG, IgM; HIV • Genetics—CF (mutations of CFTR gene) and primary ciliary dyskinesia • Pregnancy—11 to 32% of women suffer pregnancy rhinitis • Local host factors—conflicting evidence for DNS, conchae bullosae, etc. Beware of dental infections • Micro-organisms: – S. aureus (36%) – Coagulase–ve staphylococcus (20%) – Streptococcus pneumoniae (17%) • Osteitis—animal studies only—may explain resistance to ABx • Environmental: • Iatrogenic: • Helicobacter pylori and LPR—DNA detected in 11 to 33% of CRS patients—causal? • Polyps present in 0.5 to 4.3% of the population; only two-third seek medical advice • Allergy—varying reports between 10 and 81% • Asthma—31 to 42% of patients with NPs (7% of asthmatics have NPs) • Aspirin sensitivity—36 to 96% have CRS with NPs • Genetics: • Environmental factors—unclear • Day care • Nasal obstruction • Passive smoking • Bottle-feeding • Urban atmospheric pollution • Tonsillitis (immunological deficiency) • OME (immunological deficiency) • Ciliary dyskinesia, e.g., CF, primary ciliary dyskinesia • Elevation of IL-1, IL-6, IL-8 • Neutrophils—source of IL-8 and TNF-α • Expression of intracellular adhesion molecule 1 (ICAM-1) • T lymphocytes—stimulated by IL-1 and 6, TNF-α • Neutrophils predominate • Small numbers of eosinophils, mast cells, basophils • Mucosal changes: • CD4+ TH cells—initiate and regulate inflammation • Macrophages (CD68+ cells) increase • Mast cell numbers raised • Cytokine mediators: IL-1, 3, 6 and 8; tumour necrosis factor-α (TNF-α), GM-CSF, ICAM-1, MPO, and eosinophil cationic protein (ECP)—the latter is the main difference from ARS • IFN-γ and TGF-β = TH 1 pathway; TGF-β expression higher than CRS with NPs • Chemokines, e.g., CCR4+ • Eicosanoids—COX-2 mRNA and PGE2 higher than CRS with NPs • Metalloproteinases—low MMP-9 activity • Nasal nitric oxide (nNO) shows increase the correlates with subjective and objective measures of improvement • Neuropeptides such as VIP may play a role • Mucins—MUC5AC and MUC5B increased in CRS • Increased vascular endothelial growth factor (VEGF) • Biofilms—structured specialized communities of adherent micro-organisms encased in a complex extracellular polymeric substance (EPS) • Eosinophils present in 80% = marker of inflammation in CRSwNPs • Increased numbers of T cells and plasma cells • S. aureus superantigens interact with T cells in 35% • Macrophages increased with an increase in macrophage mannose receptors in polyps • Mast cells—more often IgE+ • Increased neutrophils • Overexpression of MUC8 mRNA and downregulation of MUC5AC mRNA expression—alters mucus composition • Cytokines and chemokines—differences from CRSsNPs: • Adhesion molecules—ICAM-1 among others expressed on polyp surface • Leukotrienes and their receptors unregulated in NP tissue • S. aureus enterotoxins induce a more severe eosinophilic inflammation and cause multiclonal IgE synthesis • In CF—very prominent neutrophilic inflammation • Aspirin sensitivity—inhibition of cyclooxygenase-1 causing release of lipid and non-lipid mediators • IgE+ cell numbers raised in patients with allergic, fungal, and eosinophilic CRS • Fungal-specific IgG and IgA higher in CRS with eosinophilic mucus • Endoscopy • Endoscopic-guided nasal swabs—87% accurate • CT scan (± MRI where neoplasia suspected) • Lund–Mackay scoring system for CT: • Saccharin test for mucociliary clearance—useful if normal (<35 minutes) • Ciliary beat frequency (>8 Hz for IT = normal) and electron microscopy for PCD • Nitric oxide: • Nasal airway—PIFR/acoustic rhinometry/rhinomanometry/nasal spirometry • Olfactory testing—see Chapter 34 • Aspirin challenge • QoL questionnaires—SF-36, RSOM, SNOT-22, RSDI, RQLQ, et al. • Oral ABx—after 5/7 • Topical corticosteroid • Oral corticosteroid—if severe to reduce pain • Oral antihistamine—if atopic • Decongestant • Oral antibiotics—after 5/7 • Topical corticosteroids • Saline douching • Long-term ABx (>12/52)—low-dose macrolide, e.g., clarithromycin (if IgE not elevated) • Topical steroids • Saline douching (There is a paucity of data to support postoperative management) • Oral antibiotics for 1 to 2 weeks if pus seen, but long-term ABx also recommended • Topical steroids • Short-term oral steroids • Nasal douching • Oral ABx >12/52 for late relapse—consider doxycycline • Topical/oral steroids—as guided by VAS • Nasal douche • Oral antihistamine—if atopic • As for CRSsNPs postop • Oral ABx • Topical steroids • Saline douching • PPI • Consider the role of:
24.1 Definitions
 Nasal blockage/obstruction/congestion or nasal discharge + at least one of:
Nasal blockage/obstruction/congestion or nasal discharge + at least one of:
 In addition, endoscopic and/or CT changes required to confirm symptoms above of acute rhinosinusitis (ARS)/chronic rhinosinusitis (CRS)
In addition, endoscopic and/or CT changes required to confirm symptoms above of acute rhinosinusitis (ARS)/chronic rhinosinusitis (CRS)
 <12 weeks = acute
<12 weeks = acute
 >12 weeks = chronic
>12 weeks = chronic
 Symptom-free intervals (complete resolution) but >12 weeks in total = recurrent acute
Symptom-free intervals (complete resolution) but >12 weeks in total = recurrent acute
 <10 days = common cold (viral upper respiratory tract infection, i.e., URTI)
<10 days = common cold (viral upper respiratory tract infection, i.e., URTI)
 Increase in Sx after 5 days OR persistence of Sx after 10 days = non-viral ARS
Increase in Sx after 5 days OR persistence of Sx after 10 days = non-viral ARS
 Severity defined by VAS (0–10)—“How troublesome are your Sx of ARS/CRS?”:
Severity defined by VAS (0–10)—“How troublesome are your Sx of ARS/CRS?”:
 ARS:
ARS:
 CRS:
CRS:
24.2 Aetiology
24.2.1 Acute Rhinosinusitis
 Bacteria
Bacteria
24.2.2 Chronic Rhinosinusitis without Polyps
 Bacteria—pathogens or colonizers?
Bacteria—pathogens or colonizers?
 Fungi—colonize only or promoters of allergic/eosinophilic response?
Fungi—colonize only or promoters of allergic/eosinophilic response?
 Smoking
Smoking
 Low income
Low income
 Atmospheric pollutants—no convincing evidence
Atmospheric pollutants—no convincing evidence
 Mucoceles associated with previous ESS
Mucoceles associated with previous ESS
 Recirculation of mucus from natural to surgical ostia
Recirculation of mucus from natural to surgical ostia
24.2.3 Chronic Rhinosinusitis with Nasal Polyps
 14 to 52% have +ve family history
14 to 52% have +ve family history
 Twin studies do not show that both develop NPs
Twin studies do not show that both develop NPs
 HLA associations, e.g., A74, DR7
HLA associations, e.g., A74, DR7
 Gene polymorphisms
Gene polymorphisms
 Multiple gene expressions for immune modulation
Multiple gene expressions for immune modulation
 Cystic fibrosis
Cystic fibrosis
24.3 Children
24.4 Inflammatory Mechanisms
24.4.1 Acute Rhinosinusitis
24.4.2 CRS without NPs
 BM thickening
BM thickening
 Goblet cell hyperplasia
Goblet cell hyperplasia
 Subepithelial oedema
Subepithelial oedema
 Mononuclear cell infiltration
Mononuclear cell infiltration
24.4.3 CRS with NPs
 IL-5 and IgE = CRS with NPs (TH2)
IL-5 and IgE = CRS with NPs (TH2)
 Exaggerated humoral and cellular response to airborne fungi
Exaggerated humoral and cellular response to airborne fungi
24.5 Investigations
 0 to 2 score for each of maxillary, ant. ethmoid, post. ethmoid, sphenoid, frontal
0 to 2 score for each of maxillary, ant. ethmoid, post. ethmoid, sphenoid, frontal
 Score of 0 or 2 for OMCs
Score of 0 or 2 for OMCs
 Max. score = 24 (12 each side)
Max. score = 24 (12 each side)
 LRT = <20 ppb
LRT = <20 ppb
 Nose = 400 to 900 ppb
Nose = 400 to 900 ppb
 Sinuses = 20 to 25 ppm
Sinuses = 20 to 25 ppm
24.6 Recommended Treatment Regimes
24.6.1 Adults with ARS
24.6.2 Children with ARS
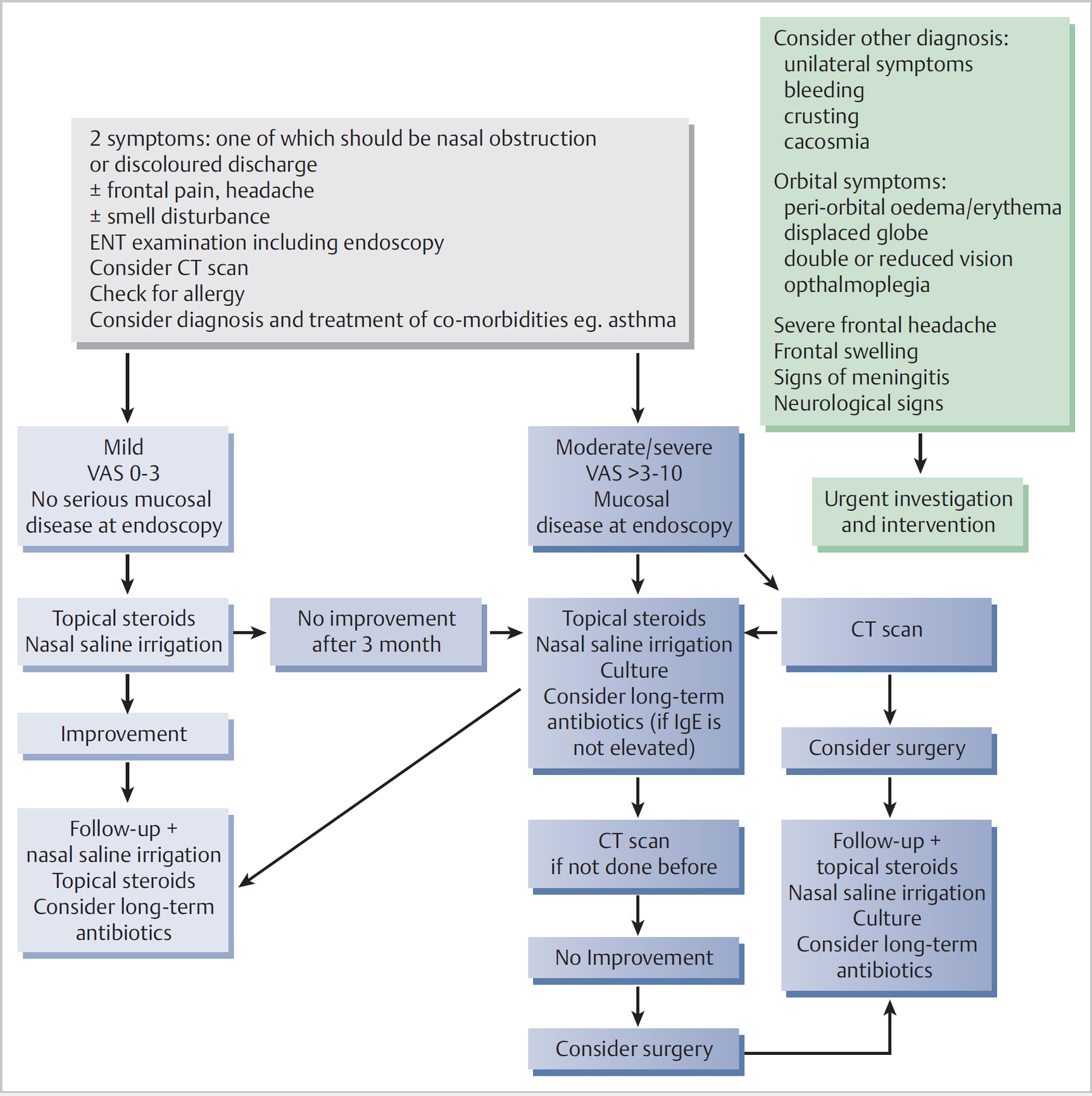
24.6.3 Adults with CRS without NPs (Fig. 24.1)
24.6.4 Adults with CRS without NPs Postop
24.6.5 Adults with CRS with NPs (Fig. 24.2)
24.6.6 Adults with CRS With NPs Postop
24.6.7 Children with CRS (Fig. 24.3)
24.7 Future Research Needs and Priorities
 Socio-economic status
Socio-economic status
 Severity staging with respect to QoL
Severity staging with respect to QoL
 Prognostic Sx in primary care
Prognostic Sx in primary care
 Endotyping and phenotyping—including how to assess this and the impact upon management and outcomes
Endotyping and phenotyping—including how to assess this and the impact upon management and outcomes
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


