Epikeratoplasty
Michael D. Wagoner
Ali A. Al-Rajhi
Epikeratoplasty was originally introduced by Dr. Herbert Kaufman (1) at the Jackson Memorial Lecture at the American Academy of Ophthalmology as an extension of the pioneering work of Joaquin Barraquer (2) in the development of keratophakia for aphakia and keratomileusis for myopia. Both of the Barraquer procedures require dissection and removal of a portion of the central cornea, technically challenging cryolathing, and expensive equipment (2). Epikeratoplasty is performed by suturing a commercially cryolathed corneal “lenticule” with specific dioptric power onto de-epithelialized central cornea without disturbance of the anterior stroma (3,4). It provides the refractive benefits of the Barraquer procedures, but with less technical complexity, cost, and risk of central corneal scarring.
Epikeratoplasty was originally introduced for contact lens intolerant, monocularly aphakic adults, in whom secondary intraocular lens implantation was contraindicated (1). The indications were later expanded to include the correction of keratoconus (5,6), pediatric aphakia (7,8), adult aphakia (9, 10, 11, 12), and myopia (13). Between 1985 and 1988 a nationwide study involving 234 ophthalmologists was conducted to evaluate prospectively the safety and efficacy of epikeratoplasty for each of these indications (13, 14, 15, 16, 17).
SURGICAL TECHNIQUE
Epikeratoplasty lenticules are prepared from corneal tissue that meet the criteria of the Eye Bank Association of America for transplantation, but do not qualify for use for penetrating keratoplasty due to factors such as poor endothelial cell counts, long death-to-preservation times, or excessive length of storage. The tissue is treated with a water-soluble green dye to aid in visualization and cryolathed to a specific dioptric power based on the patient’s spherical equivalent corrected to the corneal plane (with the exception of keratoconus, which was lathed to plano power). It may then be placed in standard corneal storage media or lyophilized prior to shipment to the operating surgeon. The lenticules are processed under environmental conditions similar to other donor corneal tissue and are not sterile. They may be obtained from Cryo-Optics (Houston, TX) or the Keratec Eye Bank (St. George’s Hospital Medical School, London, UK).
Epikeratoplasty may be performed with general anesthesia, retrobulbar or peribulbar anesthesia, or topical anesthesia (in extremely cooperative adults). The central corneal epithelium is debrided at least 1 to 1.5 mm beyond the edge of the anticipated trephination with a dull spatula, facilitated by topically applied 4% cocaine, if necessary. The use of topical alcohol should be avoided because it may contribute to poor postoperative epithelial healing, especially if limbal stem cells are damaged. All epithelia should be removed from the surgical field and fornices to prevent accidental retention of epithelial nests in the interface during lenticular suturing.
After epithelial removal, a Hessburg-Barron trephine is centered on the visual axis, and trephination is performed approximately 200 to 225 μm into the corneal stroma. A 7-mm trephine is used for aphakia and myopia, and an 8.5-mm trephine is used for keratoconus. For eyes with aphakia or myopia a 1-mm lamellar “pocket” is dissected from the base of the trephination into peripheral cornea. No lamellar dissection is required for eyes with keratoconus. Many surgeons perform an annular keratectomy of approximately 0.5 mm in diameter on the inner aspect of the trephine incision, although this is not mandatory.
Nonlyophilized tissue that has been stored in standard corneal storage media containing antibiotics may be transferred directly to the recipient eye. Lyophilized tissue is rehydrated in balanced salt solution to which an appropriate antibiotic, such as gentamicin, has been added for at least 20 minutes before use. A “refractively neutral” suture technique is used to suture an 8.5-mm donor lenticule in eyes with myopia (13) and aphakia (15, 16, 17). A 10-0 nylon needle is passed through the 130-μm thick wing of the lenticule and then into the apex of the peripheral lamellar dissection pocket. The sutures are loosely tied to avoid excessive tension on the graft and minimize risk of undercorrection of myopia and overcorrection of aphakia. Although several different sutures techniques have been tried, the use of 16 interrupted 10-0 nylon sutures has become the preferred technique. Some surgeons advocated a “no-stitch” technique
for myopic and aphakic epikeratoplasty (18), but this did not gain popular acceptance.
for myopic and aphakic epikeratoplasty (18), but this did not gain popular acceptance.
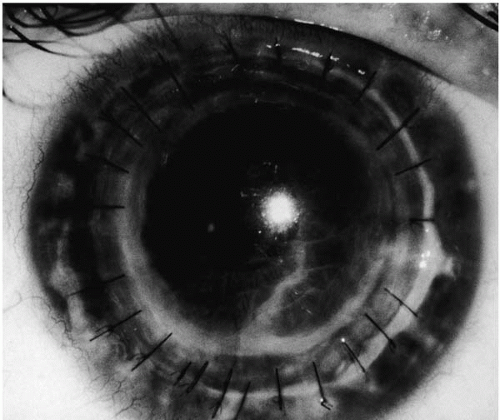 FIGURE 72-1. Epikeratoplasty for keratoconus, 1 day postoperative. Twenty-four tight 10-0 nylon sutures have been used to maximize corneal flattening, as demonstrated by the marked folds in Descemet’s membrane. |
A “corneal flattening” suture technique is used to tightly suture a 9-mm, plano donor lenticule of approximately 0.3 mm thickness in eyes with keratoconus (14). A total of 16 or 24 sutures interrupted 10-0 nylon sutures are placed, using edge-to-edge approximation. To obtain maximum flattening of the cone, some surgeons utilize a 9-0 silk suture for the four cardinal sutures and replace them with 10-0 nylon sutures at the conclusion of the case. These sutures are tied as securely as possible while the assistant flattens the cone with a flat spatula. Folds should be present in Descemet’s membrane at the conclusion of the procedure, indicating that the cone has been flattened significantly (Fig. 72-1). They vanish after suture removal (Fig. 72-2).
POSTOPERATIVE MANAGEMENT
The success of epikeratoplasty is highly dependent on facilitating prompt reepithelialization of the lenticule, especially when lyophilized tissue is used. Despite the use of pressure patching or soft contact lens therapy, epithelial defects persisting more than 2 weeks are not uncommon after epikeratoplasty. In 405 cases of epikeratoplasty performed at the King Khaled Eye Specialist Hospital (KKESH) between 1987 and 1997, persistent epithelial defects occurred in 4 (2.5%) of 161 eyes with keratoconus, 5 (4.1%) of 123 children with aphakia, and 6 (5%) of 121 adults with aphakia. A study from the Massachusetts Eye and Ear Infirmary demonstrated that placement of a temporary tarsorrhaphy at the conclusion of the surgical procedure reduced the mean time of reepithelialization to 4.61 days, compared to 8.03 days with pressure patching (p < .01) and 13.2 days with bandage soft contact lenses (p < .005) (19). Because delayed reepithelialization of 2 weeks or longer is often associated with irreversible loss of lenticular clarity, prophylactic placement of a temporary suture tarsorrhaphy at the conclusion of every epikeratoplasty procedure has now become routine practice.
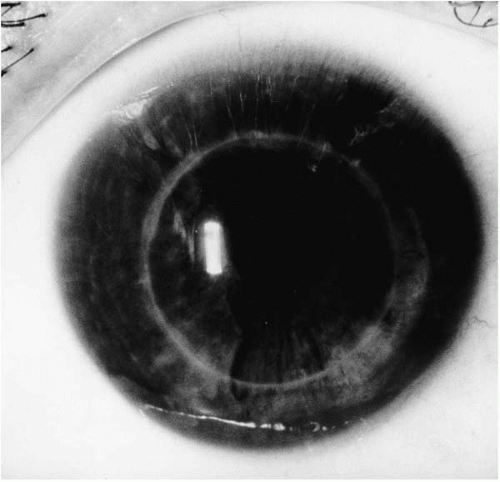 FIGURE 72-2. Epikeratoplasty for keratoconus, 2 year postoperatively. Excellent flattening of the cone has been achieved and maintained, with excellent interface clarity. The folds in Descemet’s membrane have completely disappeared. |
Removal of the epikeratoplasty lenticule is occasionally necessary in the early postoperative period (13, 14, 15, 16, 17,20, 21, 22, 23, 24, 25, 26, 27, 28, 29). Graft removal is highly recommended when delayed reepithelialization results in loss of graft clarity and a poor visual result. In almost every case, lenticule removal under these circumstances is associated with complete reversal of the original status of the recipient cornea. Graft removal is mandatory when delayed reepithelialization is associated with sterile ulceration or secondary microbial keratitis, which may extend into the recipient cornea and produce permanent scarring (24, 25, 26, 27).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


