Endoscopic septoplasty has gained popularity since Lanza and colleagues and Stammberger first described the technique. This technique has several advantages over the traditional “headlight” septoplasty. These advantages include superior visualization, accommodation of limited and minimally invasive septoplasty, and usefulness as an effective teaching tool. This article reviews and illustrates the endoscopic septoplasty technique and discusses its limitations and advantages.
Septoplasty is one of the most common procedures performed in otolaryngology. Modern septoplasty techniques were initially described by Killian and Freer in the early twentieth century. Indications for septoplasty are broad, and include correction of septal deviation resulting in nasal obstruction, the need for improved access during endoscopic sinus surgery (ESS) or endoscopic dacrocystorhinotomy, and treatment of facial pain/headaches associated with septal spurs contacting the lateral nasal wall. Septoplasty is classically performed under direct visualization using a headlight and nasal speculum. However, a newer technique using endoscopic visualization and instrumentation has gained widespread popularity and acceptance following several reports of favorable outcomes.
Endoscopic septoplasty was initially described by Lanza and colleagues and Stammberger in 1991. Early reports of endoscopic septoplasty describe several advantages associated with the technique. For example, the technique makes it easier for surgeons to see tissue planes. Also, because the technique is minimally invasive, it offers a better way to treat isolated septal spurs. Furthermore, the technique gives surgeons improved access to a deviation that is posterior to a septal perforation. Additionally, the endoscopic approach makes it possible for many people to simultaneously observe the procedure on a monitor, making the approach useful in a teaching setting. Nasal endoscopy is a valuable tool for initial assessment of the relationship of the septum to the middle turbinates, which allows the surgeon to judge whether or not the position of the septum will limit access during ESS. Even in the absence of subjective nasal obstruction or gross septal deviation, septoplasty may be necessary to maximize access to the middle meatus during ESS, such as in the setting of a narrow nasal cavity with a prominent septal body ( Fig. 1 ). Nasal endoscopy is an excellent tool for outpatient surveillance following septoplasty during the initial postoperative healing period and beyond.
Nasal septum function and anatomy
The nasal septum lies in the sagittal plane and separates the nasal cavity into two sides. In most cases, the bony or cartilaginous septum deviates to some degree from the midline. Such deviations may be congenital or acquired. Septal deviations may be broad and convex (often termed bowing ) or sharp and acute (often termed spurring ). The septal mucosa often becomes very thin over the apex of a spur, which is an important consideration during septoplasty. The cartilaginous septum is formed by the quadrangular cartilage anteriorly, while the bony septum comprises vomer posteriorly and the perpendicular plate of the ethmoid posterosuperiorly. The septum sits atop the midline crest of the maxilla anteriorly and the palatine bone posteriorly. The septum is bordered anterosuperiorly by the paired nasal bones and upper/lower lateral nasal cartilages, superiorly by the cribriform plate and floor of the frontal sinus, and posterosuperiorly by the face of the sphenoid. The vomer thickens considerably at the posterior aspect of the septum, where it terminates at the junction with the nasopharynx.
The nasal septum is lined with ciliated columnar respiratory epithelium, which transitions to squamous epithelium within several millimeters of the collumella. The vascular supply to the septum is robust, and is provided by branches of the sphenopalatine, anterior ethmoid, posterior ethmoid, greater palatine, and superior labial arteries. The septum works in conjunction with other structures within the nasal cavity to warm and humidify inspired air, while directing air and mucus posteriorly toward the nasopharynx.
Technique
Drawbacks of Traditional Septoplasty
Traditional septoplasty is performed under direct visualization using headlight illumination and a nasal speculum. Visualization is limited with this technique, and the relation of the nasal septum to the lateral nasal wall structures is difficult to determine. The posterior septum is particularly difficult to visualize with this technique because of the narrow field of view and limited illumination. However, instrumentation is relatively simple, and a surgeon experienced in the technique can perform it rapidly.
Advantages of Endoscopic Septoplasty
Endoscopic septoplasty is associated with several distinct advantages over traditional septoplasty. The endoscopic technique provides the benefit of magnification, which the traditional headlight technique does not offer. In addition, illumination and visualization is better with the endoscopic technique than with the headlight technique. With the endoscope, it is possible to see the separation of collagenous fibers connecting the perichondrium and periostium to underlying bone and cartilage during surgical dissection. Mucosal disruptions are recognized immediately, and their size may be controlled using careful and meticulous dissection. Bleeding is minimized using injection of lidocaine with epinephrine, and optimal visualization is obtained with use of a suction Freer elevator. Endoscopic views of the nasal cavity are more natural than with the traditional headlight/speculum technique, since the nasal speculum causes some distortion of normal nasal anatomy.
One distinct advantage of the endoscopic approach is that it enables many people to observe the procedure on a monitor. This is very useful in a teaching setting, where it offers a convenient way for residents and students to directly observe the procedure, and a useful tool for a teaching surgeon to closely observe a resident. Operating room personnel may also observe the procedure and more accurately predict the next step in the case.
Endoscopic septoplasty may be performed using traditional ESS instrumentation. Because of this and because both endoscopic septoplasty and ESS involve the same field, endoscopic septoplasty can be performed in conjunction with ESS. This is important because concomitant septoplasty during sinus surgery may be necessary to provide the best access to the middle meatus. Suboptimal access during ESS leads to poor visualization, thereby increasing the likelihood of surgical complications or poor surgical outcomes. In some cases, uncorrected septal deviation increases the likelihood of middle turbinate lateralization and may lead to poor visualization during postoperative endoscopic examination.
Description of Endoscopic Septoplasty Technique
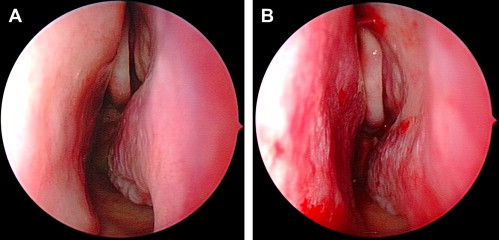
Little additional instrumentation is required when endoscopic septoplasty is performed in conjunction with ESS ( Fig. 2 ). Before the procedure, the nasal mucosa is decongested with topical epinephrine, oxymetazoline, or cocaine. The nasal cavity is examined using a 0° endoscope. The location and degree of septal deflection or spurring is noted. If ESS is planned, the position of the septum to the middle turbinates is noted. A useful landmark is the axilla of the middle turbinate where it attaches anteriorly and superiorly to the lateral nasal wall. If the axilla is not easily visualized, the surgeon may have difficulty with access and visualization during ESS or in the postoperative period. In a narrow nasal cavity, the septal mucosal flaps may be “retracted” following septoplasty, allowing for improved endoscopic access and visualization ( Fig. 3 ). An additional consideration is the superior aspect of the septum and septal body. While not usually deviated, this portion of the septum tends to be thicker than other parts of the septum, thus narrowing the nasal cavity and limiting access to the middle meatus.

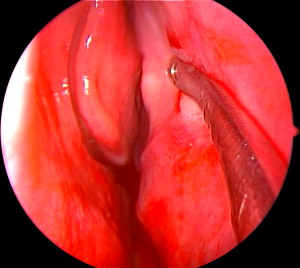
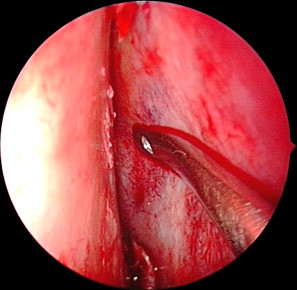
One-percent lidocaine with 1:100,000 units of epinephrine is injected along both sides of the septum in a subperichondrial plane. A Killian incision is made on the left side of the caudal septum at the mucocutaneous junction. A Cottle elevator is then used to develop a submucoperichondrial plane along the left side of the septum. Further dissection in a posterior direction is performed using the suction Freer elevator ( Fig. 4 ). When elevating the mucosa over spurs, care is taken to prevent mucosal tears due to thinning of the mucosa. The septal cartilage is then sharply scored and incised, leaving at least 1 cm of caudal and dorsal septum for nasal tip support ( Fig. 5 ). A submucoperichondrial plane is then developed on the opposite side of the septum. Once the septal cartilage and bone is isolated from the mucosa, the Jansen-Middleton punch is used to incise the septum in an anterior to posterior manner ( Fig. 6 ). The Takahashi forceps are then used to remove all deviated portions of the bone and cartilage in a twisting motion. The endoscope is used throughout the procedure, and may be placed between the mucosal flaps or within the nasal cavity to ensure correction of all septal deformities. The mucosal flaps are reapproximated and the Killian incision is closed using a 4-0 chromic gut suture. A 4-0 Vicryl rapide suture is used to further reapproximate the flaps in a quilting fashion. If a perforation is not present in one of the mucosal flaps, a drainage port is created posteriorly and inferiorly to allow for dependent drainage and to avoid development of a septal hematoma. Nasal packing and splints are used only in special cases (see Fig. 3 ).