Endoscopic Reduction of Orbital Blow-Out Fracture
Hiroshi Moriyama
INTRODUCTION
Fractures of the floor of the orbit have long been known to be more common than are fractures of the medial wall of the orbit. However, fractures of the medial wall are not uncommon and can now be easily diagnosed with computed tomography (CT).
In the past, there were three surgical approaches to fractures of the medial wall of the orbit: (a) the transorbital approach through an external incision, (b) the maxilloethmoidal approach, and (c) the endonasal approach. Most publications in the 1970s reviewed techniques for the transorbital approach, such as an incision over the medial canthus, medial brow incision, and the conjunctival approach. The combined transorbital and maxilloethmoidal approach was used sometimes. However, the endoscopic endonasal surgery now allows direct access, clear visualization, and precise surgical procedures to repair fractures of the medial orbital wall.
Conventional surgical treatment of fractures of the floor of the orbit by ophthalmologists and plastic surgeons involves microscopic transorbital reduction through an incision in the inferior eyelid or conjunctiva. However, the use of rigid endoscopes has allowed fractures of the orbit to be treated via less-invasive endonasal or transmaxillary routes for endoscopic sinus surgery.
Fractures of the medial wall or floor of the orbit can restrict ocular motility and cause enophthalmos. Fractures of the orbit can easily be recognized with such imaging methods as CT and magnetic resonance imaging (MRI).
In my experience, the endoscopic endonasal approach allows direct access, clear visualization, and precise surgical procedures in the treatment of fractures of the medial wall of the orbit. Furthermore, endoscopic endonasal surgery with or without transmaxillary repair is an effective and less-invasive method for treating fractures of the floor of the orbit.
Fractures of the floor of the orbit are divided into two types. One type is a wide fracture called a blowout fracture (BOF), and the other is a linear fracture called a trapdoor fracture in which bone fragments are not displaced. However, severe restriction of ocular motility frequently occurs with trapdoor fractures due to entrapment of the inferior rectus muscle. Therefore, early surgical treatment is required for trapdoor fractures to free herniated orbital tissue entrapped by fractured bone and to restore full ocular motility. If a trapdoor fracture is suspected, it should be repaired within 1 week after injury to prevent cicatrization of intraorbital tissue.
In my experience, endoscopic repair is a useful, safe, and effective operative technique for treating fractures of the orbit. However, the postoperative prognosis is often unclear, and the patient must be adequately informed about possible outcomes before surgery.
Types of Fractures of the Orbit
Fractures of the orbit are divided into three types: (a) fractures of the orbital floor, which are the most common; (b) fractures of the medial wall of the orbit (lamina papyracea); and (c) combined fractures of both the floor and
medial wall of the orbit. In the 1990s, 229 orbital fractures were treated with endoscopic endonasal surgery in our department: 108 (47%) were fractures of the floor of the orbit, 64 (28%) were fractures of the medial wall, and 57 (25%) were combined fractures of both the floor of the orbit and the medial wall.
medial wall of the orbit. In the 1990s, 229 orbital fractures were treated with endoscopic endonasal surgery in our department: 108 (47%) were fractures of the floor of the orbit, 64 (28%) were fractures of the medial wall, and 57 (25%) were combined fractures of both the floor of the orbit and the medial wall.
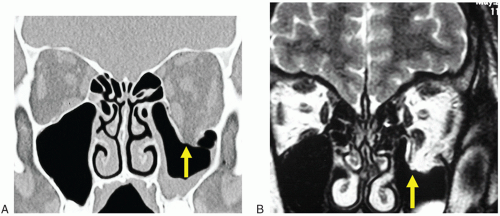 FIGURE 34.1 A and B: CT and MRI image of blow-out fracture (extensive fracture type of the floor of the orbit (arrow). |
BOFs are the most common type of fracture of the floor of the orbit, accounting for 70% of cases (Fig. 34.1), and trapdoor fractures are less common, accounting for 30% of cases (Fig. 34.2). In BOFs, intraorbital tissue can be displaced into the maxillary sinus but cannot be entrapped between fragments of fractured bone. In contrast, severe restriction of ocular motility often occurs in trapdoor fractures despite the minimal findings on CT, because herniated extraocular muscles, adipose tissue, and fibrous tissue from the orbit are entrapped between the edges of fractured bone.
The age range of our 229 patients was 4 to 74 years. Young patients tended to have fractures of the orbital floor, whereas adults tended to have fractures of any type. Furthermore, among patients with fractures of the floor of the orbit, young patients are more likely to have trapdoor fractures (Fig. 34.3).
HISTORY
The symptoms of orbital fractures include diplopia, restriction of ocular motility, pain on ocular movement, eye strain, and palpebral swelling. If a fracture of the orbit is suspected on the basis of a history of orbital injury and clinical features, diagnostic imaging and ophthalmologic examination should be performed (Fig. 34.2).
PHYSICAL EXAMINATION
Ecchymosis of the soft tissues is usually noted. Visual acuity and visual fields should be evaluated. The traction test (forced duction test) should be performed to determine whether extraocular muscles have been entrapped by the edges of a fracture. The range of motion of the globe should be tested. The Hess test should be performed to evaluate ocular motility.
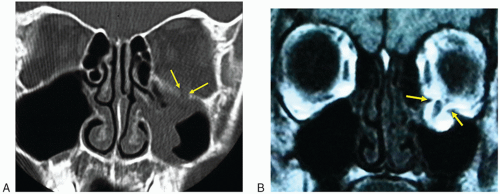 FIGURE 34.2 A and B: CT and MRI image of trapdoor fracture (linear fracture type) (arrows). |
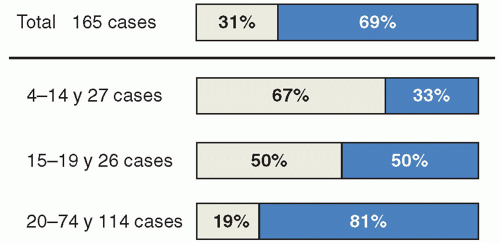 FIGURE 34.3 Relation between types and age of orbital floor fracture. |
INDICATIONS
The indications for and timing of surgery for fractures of the orbit are controversial. Generally, surgery for a fracture of the orbit is indicated when the following three criteria are met: (a) diplopia on ophthalmologic examination, (b) fracture of the orbit confirmed with CT or MRI, and (c) no improvement in symptoms after 1 week of conservative treatment.
Smith and Regan noted that early surgical treatment tends to prevent subsequent permanent deformity. If the interval from injury to surgery is 4 weeks or more, traumatic pathologic changes, such as fibrosis and adhesion, can occur with poor long-term results.
For trapdoor fractures causing diplopia, early surgical treatment is needed to free the orbital tissues entrapped by fragments of fractured bone and to restore ocular motility.
For fractures of the medial wall without limitations of ocular motility, surgery is indicated only if secondary frontal sinusitis might later be caused by obstruction of the frontonasal drainage pathway as a result of herniated orbital contents.
Recent clinical studies have recommended prompt surgical repair in patients with large fractures (involving >50% of the floor of the orbit) and in those with diplopia or enophthalmos of greater than 2 mm within 7 to 10 days after injury.
For fractures of the floor of the orbit, the choice of the endoscopic endonasal approach or the combined endoscopic endonasal and transmaxillary approach depends on the location of the fracture and whether orbital tissue has been displaced laterally or medially. The endoscopic endonasal approach should be used when the center of the fracture is medial to the infraorbital nerve or when the orbital tissue is herniated medially. The combined approach should be used for cases in which other conditions are present and for cases of extended mixed fracture.
If the orbital tissue is herniated laterally, the endoscopic transmaxillary approach is indicated because bone fragments (arrow




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
