Partial Septectomy and Sphenoidotomies
Richard J. Harvey
INTRODUCTION
Endoscopic endonasal access to the sphenoid sinus is a common maneuver for a variety of inflammatory and neoplastic pathologies. There are three variations of wide sphenoid access that I employ in my surgery, and these are discussed below. This chapter focuses on the surgical technique to access the sphenoid widely so that the entire width of the sphenoid cavity is exposed from lateral wall to lateral wall. This chapter is about the procedure not the pathology, so I will discuss the key elements of the history, physical examination, and investigations that are important when developing this corridor to the sphenoid sinus. The variety of inflammatory sinus, pituitary, and skull base pathologies addressed via a transsphenoid approach is very broad, and I have chosen to discuss the nuances of the approach to allow for reconstruction as part of the approach in some skull base pathologies.
HISTORY
The essential preoperative history should focus on factors that will affect recovery, reconstruction, and the potential of surgery to make preexisting conditions worse. Inflammatory airway conditions such as rhinitis and asthma predispose to the development of a marked postoperative inflammatory response. The surgery can act as a major inflammatory trigger, and perioperative corticosteroids should be considered to ensure that the mucosa will have a good recovery postoperatively. Smoking cigarettes and other forms of smoking will negatively affect the recovery of the mucosa. When performing an endonasal access for nonsinus conditions (such as pituitary and intracranial lesions), the patient should not smoke for 6 weeks prior to surgery and for 6 weeks after surgery.
The patients’ dexterity and their ability to perform postoperative care tasks such as nasal irrigations should be assessed. Significant crusting can occur after extensive procedures to remove tumors from the sphenoclival area. The hand power required to use a high-volume positive pressure irrigation device such as a squeeze bottle is critical to good recovery. Alternatives, such as neti pots, require good mobility of the neck and head. Powered irrigation devices might need to be provided to those not capable of performing these tasks.
Importantly, knowledge of prior septal, turbinate, and sphenoid surgery is important to define the reconstructive options available if transdural surgery is undertaken. Prior wide unilateral sphenoidotomy may have already sacrificed the ipsilateral branch of the septal artery. A prior sphenopalatine ligation will have compromised a septal flap pedicle upstream, and a prior turbinate procedure may make the inferior turbinate flap unusable. Although a prior septoplasty or septal reconstruction may not prevent a good septal flap harvest, especially if the original surgeon was in the correct subperiosteal plane, it is good to have a backup option if the flap cannot be successfully raised. Prior radiation therapy will usually make healing slower and the need for a vascular flap even more important.
It is critical to establish preexisting olfactory dysfunction. Almost all patients with a wide bilateral sphenoid approach will lose their olfaction temporarily. The resection of the inferior half of the superior turbinate might compromise olfaction and near-complete resection of the superior turbinate as occurs in a transplanum
approach even more so. Clinical research has shown that patients recover their sense of smell as the loss is temporary and associated with postoperative inflammatory changes rather than critical reduction of the olfactory mucosa. Patients should, however, be warned of this phenomenon, and those with olfactory disturbance may be better served by an alternate route if the approach may cause the function to deteriorate further. Meningioma of the sphenoid planum is a good example. If a transnasal route is used and the patient has an excellent outcome but is significantly hyposmic or anosmic, then a supraorbital keyhole craniotomy approach may have been a better choice.
approach even more so. Clinical research has shown that patients recover their sense of smell as the loss is temporary and associated with postoperative inflammatory changes rather than critical reduction of the olfactory mucosa. Patients should, however, be warned of this phenomenon, and those with olfactory disturbance may be better served by an alternate route if the approach may cause the function to deteriorate further. Meningioma of the sphenoid planum is a good example. If a transnasal route is used and the patient has an excellent outcome but is significantly hyposmic or anosmic, then a supraorbital keyhole craniotomy approach may have been a better choice.
PHYSICAL EXAMINATION
Preoperative endoscopic examination can identify septal deviations and allow for surgical planning. In my institution, most septal deviations are corrected at the time of the sphenoidectomy. This helps to ensure good postoperative access for immediate wound care but also for long-term surveillance of the final cavity. The septal flap is usually easier to develop on the concave side. Septal spurs may limit the side that can be harvested for a septal flap and often limit the size of the flap, as the flap is often torn during elevation. Concha bullosa of the middle turbinate may make a transethmoid approach more practical on the ipsilateral side or be reduced to allow a transnasal route. Look for evidence of prior septal, sinus, or turbinate surgery. Incidental pathology of the nose or paranasal sinuses should be excluded.
INDICATIONS
Inflammatory sinus disease: surgical salvage when prior limited unilateral procedures have failed and the need to provide an optimal cavity to allow for topical care and long-term sinus rehabilitation. Bilateral approach to the sphenoid with septectomy is the equivalent of the Draf 3 to the frontal sinus by using both sides to ensure long-term access and patency (Fig. 16.1A).
Pituitary tumors: this is the most frequent indication. Unilateral nasal approaches to address pituitary pathology are no longer practiced at my institution. Although it is acknowledged that, a unilateral, single-nostril
approach may allow some pituitary adenomas to be managed, it is extremely restrictive and limits any extended maneuvers (Fig. 16.1B).
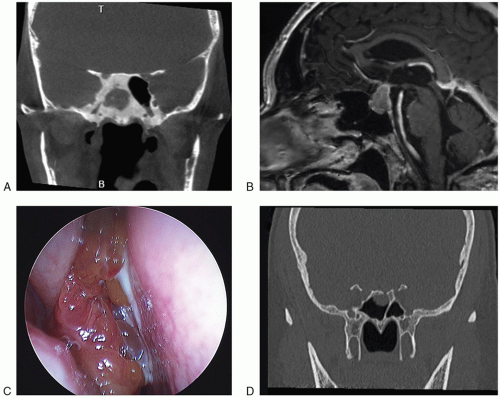
FIGURE 16.1 Typical sphenoid pathologies requiring a bilateral approach and septectomy. A: An extensive fungal ball is unlikely to function and have adequate postoperative access with such thick bone. B: Pituitary adenomas. C: Benign neoplasia such as the sphenoid inverted papilloma. D: A posttraumatic meningocele of the roof of the sphenoid.
Skull base pathologies: providing a wide exposure of the parasphenoid anatomy is the cornerstone to further expanded approaches (transplanum, transclival, subpetrous) (Fig. 16.1C).
Encephaloceles and lateral cerebrospinal fluid (CSF) leaks: wide access is often required ± transmaxillary (pterygoid) approach for very lateral locations (Fig. 16.1D).
CONTRAINDICATIONS
The general principle of surgical access is of critical importance. If the surgical approach crosses the axis of a critical neural or vascular structure, then an alternate route should be considered. For instance, tumor lateral to the bifurcation of the internal carotid (ICA) should be approached through an anterolateral craniotomy (supraorbital, orbitozygomatic, or pterional). Similarly for pathology lateral and superolateral to the optic nerve, an alternative route should be used.
Active sinusitis should be a relative contraindication when using this technique for skull base pathologies. Preoperative antibiotic therapy should be given in cases where the bacterial colonization is associated with the pathology. Severe local mucosal involvement from conditions such as sarcoid, Wegener’s granulomatosis, and amyloidosis warrants consideration of an alternate route.
Finally, there are very few local anatomical variations that are a contraindication. Most of the variations of sphenoid pneumatization and intersinus septum arrangements can all be managed surgically. However, a midline ICA, either as an anatomical variation or from ectasia, in conditions such as acromegaly, may make this approach difficult. An aberrant branch of the ICA branch may also warrant an alternative surgical approach.
PREOPERATIVE PLANNING
The use of both computed tomography (CT) without contrast and magnetic resonance imaging (MRI) with gadolinium contrast are useful. The CT will help to define surgical landmarks, concha bullosa, presellar sphenoid pneumatization (Fig. 16.2), and Onodi cells that may appear to limit full exposure. The MRI allows assessment of the pathology in relation to the ICA, the ICA position, and the tumor location relative to the sella, cavernous sinus, and optic nerve.
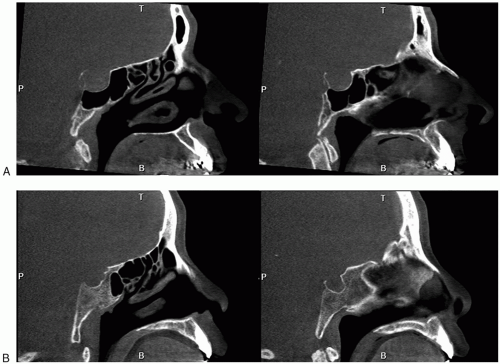 FIGURE 16.2 The pneumatization of the sphenoid is critical in planning. The postsella pneumatization of (A) allows for easy identification of sphenoid and sella anatomy; in contrast, the conchal development of (B) means that drilling is required to reach the sella as the sphenoid is small and featureless. |
Formal angiography should be considered in cases of ICA dysplasia or ectasia. The merits of preoperative balloon occlusion testing are very limited and should be applied when carotid sacrifice and bypass is being considered and not just because of the risk of bleeding from the carotid artery.
Endoscopic surgery is equipment dependent. Sphenoid surgery is often not possible without appropriate drills and bipolar diathermy devices. Instruments that are essential in some sphenoid surgeries may be found in the section entitled Instruments to Have Available.
SURGICAL TECHNIQUE
1. Preparation (with the patient under total intravenous general anesthesia)
a. 0.5-inch × 3-inch cotton pledgets soaked in 1:2,000 adrenaline + 1% ropivacaine.
i. Ten pledgets soaked by 10 mL of solution
ii. Three pledgets placed in each side of the nose immediately after endotracheal intubation
iii. Remaining pledgets join the setup for use intraoperatively during the extradural approach
b. Remove the cotton pledgets and perform the injections immediately when the endoscope is setup using a 1% ropivacaine and 1:100,000 adrenaline mixture.
i. 10-mL solution made by 9 mL of 1% ropivacaine and 1 mL of 1:10,000 adrenaline
ii. Approximately 6 to 8 mL injected via 22-g spinal needle on 10-mL syringe
1. Distal 6 mm of the needle bent at 45 degrees with bevel up to facilitate injection. The shaft is bayoneted to improve hand position
iii. Start posterior and inferior first to avoid bleeding onto the surgical field
iv. Injection: sphenoid rostrum, choana inferiorly, septum, floor of the nose, and root of the middle turbinate
c. Replace cotton pledgets under endoscopic control after injecting and complete setup of the surgical field, that is, microdebriders, bipolar forceps, check that devices are working, and check required instruments— as much time as possible.
d. Wait for the systemic effects of the injection to resolve before surgery starts. Usually when the heart rate is below 70 rather than a measure of mean arterial pressure.
2. Initial transnasal approach
a. Carefully seek out the superior meatus and create microfractures at the junction of the superior and middle turbinates superiorly. This is preferable to random lateralization of the middle turbinate as it ensures that mobilization occurs at the mechanically important location. This also avoids bleeding anteriorly.
b. Remove the inferior half or 8 mm of the superior turbinate (and supreme if necessary).



