21 Endoscopic Pituitary Surgery in the Cavernous Sinus
The history of surgical treatment of cavernous sinus (CS) tumors has had an alternating evolution; in beginning the CS was considered to be a “no-man’s land,” and all surgical approaches were avoided. In the 1960s, with the advent of the transcranial approach,1 a 20-year-long phase of enthusiasm began. Disappointment, arising from the elevated morbidity of this type of surgery, resulted in another refusal to operate on the CS.2 With the recent introduction of minimally invasive surgical techniques, combined with the changing mentality regarding the management of benign tumors of this area, our thinking is again changing. The goal is to resolve symptoms and control tumor progression without causing additional neurologic deficit. Radical removal, if associated with significant postoperative deficits, is no longer acceptable. It is better to implement a multi-modal treatment strategy in which surgery, together with radiation and pharmacologic therapy, contributes to the final result.
The endoscope represents the most recent adjunct in the century-long evolution of the transsphenoidal approach, which began by using the naked eye, evolved to incorporate magnifying glasses, and, finally in the 1970s, together with the microscope, became the approach of choice. The endoscope, thanks to its angled view and the flexibility of its surgical trajectories, has improved surgical results and has renewed interest in approaches to the CS. The endoscope improves the possibility of accessing, through an extracranial route, the lateral extension of the tumor thanks to the panoramic and angled view and peripheral magnification.3 In an anatomical study in 2001, Alfieri and Jho4 demonstrated the feasibility and the advantages of the endoscope in the endonasal approach to the CS. Three types of approaches—paraseptal, middle turbinectomy, and middle meatal—have been described, which are tailored according to the mediolateral extension of the tumor.
The Bologna group reported the first surgical series,5,6 proposing a “far-lateral” approach, the ethmoido-pterygosphenoidal endoscopic approach (EPSEA), which is appropriate for tumors also invading the lateral compartment of the CS. Another extreme lateral approach may be considered, namely the trans-maxillo-pterygoid approach, which is indicated for tumors extending from the CS through the foramen rotundum to the pterygomaxillary fossa, or vice versa. Therefore, multiple endoscopic endonasal approaches are currently available, and they should be selected and tailored according to the CS compartments involved by the tumor.
In this chapter we report our experience in endoscopic endonasal CS surgery in pituitary adenomas. We focus our attention on pituitary adenomas because they are the most representative and homogeneous group of pathologies invading the CS, and there are well-established criteria to evaluate the results, making the present series comparable with previously reported series.
 Indications for Endoscopic Endonasal Cavernous Sinus Surgery
Indications for Endoscopic Endonasal Cavernous Sinus Surgery
In agreement with many authors,1,7 we believe that the CS is an extradural vascular venous structure, in continuity with other similar structures along the craniospinal axis. Following the general surgical rule of removing extradural tumors using an extradural approach, we believe that endoscopic endonasal CS surgery should be used in CS tumors having an extradural location. The advantages of an extradural approach are multiple; it is extracerebral, avoiding any brain manipulation; the CS is penetrated through the medial wall in its sellar or sphenoidal part, which is devoid of any cranial nerves; the operation proceeds through surgical corridors with no risk (medial and posterosuperior compartments) or little risk (anteroinferior or lateral compartments) of cranial nerve damage. If there is an intradural growth, a transcranial approach, or a combined or multistaged craniotomy and endoscopic approach, is preferred.
It is of paramount importance to have adequate instrumentation and to plan the approach according to the CS compartments involved by the tumor.
 Instrumentation
Instrumentation
The instrumentation used in the endoscopic technique is a Xenon 300-W cold-light fountain source, an endoscopic video camera, and a video recorder. The endoscopes are 0-, 30-, and 45-degree Hopkins telescopes (Karl Storz, Tuttlingen, Germany), 4 mm in diameter, and 18 mm long. A cleaning system with pedal control is used to reduce the necessity of extracting the telescope from the nose every time vision becomes unclear. At the end of the approach phase and during the tumor removal phase, we use a mechanical holder for the endoscope to allow the surgeon to work with both hands. The camera zoom allows a better definition of the anatomical features, and positioning the endoscope further away from the surgical field reduces the possibility of contamination of the tip of the telescope by blood.
 Technical Adjuncts
Technical Adjuncts
Computer-assisted navigation and the micro-Doppler help to precisely localize the internal carotid artery (ICA) before the incision in the CS wall and during the tumor debulking. Modern navigation systems using a magnetic field to localize the pointer are especially suitable for endoscopy. They allow more continuous navigation, avoiding line-of-site obstruction from the body of the surgeon, or the endoscope itself coming between the pointer and the camera.
Intraoperative magnetic resonance imaging (MRI) or computed tomography scans may be extremely useful. We believe that they should be adjuncts to, and not substitutes for, the navigation system and the Doppler.
 Surgical Technique
Surgical Technique
Surgery is performed with the patient under general anesthesia using orotracheal intubation; the patient is placed in a half-sitting position with the head turned toward the surgeon resting freely in the horseshoe head-holder. The oropharynx is packed with moist gauze to prevent blood and secretions from the operative site from reaching the stomach. The nose and face are cleaned with soap and aqueous solutions. The nasal mucous membranes are decongested with 5% Xylocaine. The periumbilical abdomen is routinely prepared for the eventual harvest of a free fat graft.
Different surgical approaches can be used for pituitary adenomas involving the CS: either the midline transsphenoidal endoscopic approach (MTEA) or the EPSEA.
The approach is selected according to the compartments involved by the tumor. An MTEA is adequate when the invasion is confined to the medial and posterosuperior compartments (Figs. 21.1, 21.2, and 21.3). When the tumor invades the anteroinferior and lateral compartments of the CS or invades the entire CS, the EPSEA is required (Figs. 21.4, 21.5, and 21.6).
Midline Transsphenoidal Endoscopic Approach
The surgical procedure can be divided into three stages: approach, tumor removal, and closure.
Stage I: Approach
The lateral dislocation of the middle and upper turbinate allows the localization of the sphenoethmoidal recess and the natural ostium of the sphenoid sinus.
The opening of the sphenoid sinus starts with the enlargement of the natural ostium. The anterior sphenoidotomy should be wide, extending from the roof to the floor of the sphenoid sinus vertically and exceeding the sphenoidal ostia laterally. To gain access to the surgical field from both nostrils, 1 cm of the posterior end of the nasal septum has to be removed, using a back-biting forceps.
All the sphenoidal septa should be removed. The sphenoidal mucosa may be preserved because the wide opening of the natural ostia avoids the risk of postoperative mucocele; preserving the mucosa permits faster postoperative stabilization of the sphenoid cavity with decreased incidence of sphenoidal inflammatory sequel.
The opening of the sellar floor is performed using a drill and is enlarged using a Kerrison rongeur; it should be wide, from the superior to the inferior inter-CS and from one CS to the other (Fig. 21.7A). The bone overlying the invaded CS must be carefully removed from the opticocarotid recess to the paraclival carotid protuberance vertically and 1 cm laterally to the sella, exposing the main bulge of the parasellar carotid artery (Fig. 21.7B). This bone removal later increases the capacity of inspection of the CS content by gently displacing the anterior membranous CS wall laterally.
Stage II: Tumor Removal
The dural opening starts in the sellar area. The sellar component of the tumor is removed first. Subsequently, the medial compartment of the CS is entered, either enlarging the opening of the medial wall created by the tumor itself or (more rarely) making an incision into the medial wall in a safe area (normally located in the posterior two thirds of the medial wall of the CS) (Fig. 21.7B). Recognition of this “safe” area requires the identification of the bulging of the tumor and an accurate mapping of the course of the ICA (using direct vision, micro-Doppler, and neuronavigation) (Figs. 21.1 and 21.6) The removal of the tumor inside the medial and posterosuperior compartments of the CS is performed under direct view and has no risk of neural damage due to the absence of cranial nerves in this location (Fig. 21.8). Usually, a 0-degree endoscope is adequate for the procedure.
Stage III: Final Exploration and Closure of the Surgical Field
Hemostasis is obtained by packing with a cottonoid. At the end of the removal stage, free-hand exploration into the surgical field using angled 30- and 45-degree optic scopes is recommended.
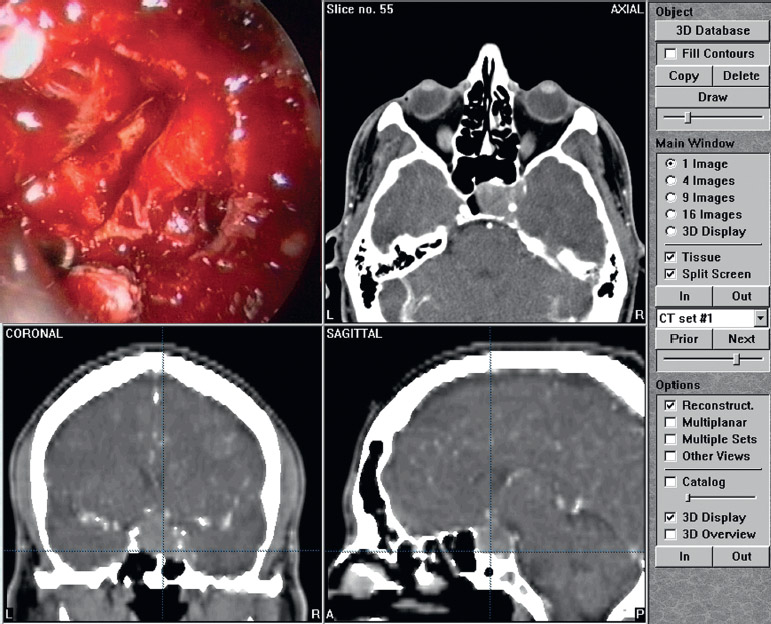
Fig. 21.1 Patient C.E. with adrenocorticotropic hormone adenoma invading the left cavernous sinus (CS) (anteroinferior compartment) and compressing the right CS. (From Fatemi N, et al. Instrumentation assessment: short trapezoidal speculums for suprasellar and infrasellar exposure in endonasal transsphenoidal surgery. Neurosurgery 2008; 62(5 Suppl2):ONS325–329. Reprinted with permission. Copyright 2008 Lippincott Williams & Wilkins.)
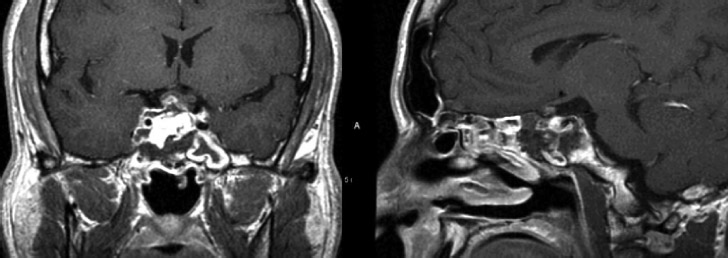
Fig. 21.2 Magnetic resonance imaging at 2-day follow-up in patient C.E. Tumor removal from the sella cavity and the anteroinferior compartment of left cavernous sinus is clearly visible. (From Mattozo CA, et al. Suboptimal sphenoid and sellar exposure: a consistent finding in patients treated with repeat transsphenoidal surgery for residual endocrine-inactive macroadenomas. Neurosurgery 2006;58:5. Reprinted with permission. Copyright 2006 Lippincott Williams & Wilkins.)
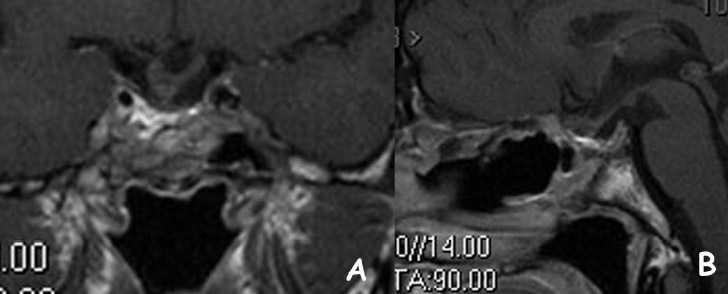
Fig. 21.3 (A,B) Magnetic resonance imaging at 6-month follow-up in patient C.E.; no residual tumor. The fat is subtotally reabsorbed and the pituitary gland is sloped downward. (From Dusick Jr, et al. Avoidance of carotid artery injuries in transsphenoidal surgery with the Doppler probe and micro-hook blades. Neurosurgery 2007;60:ONS Suppl 5. Reprinted with permission. Copyright 2006 Lippincott Williams & Wilkins.)
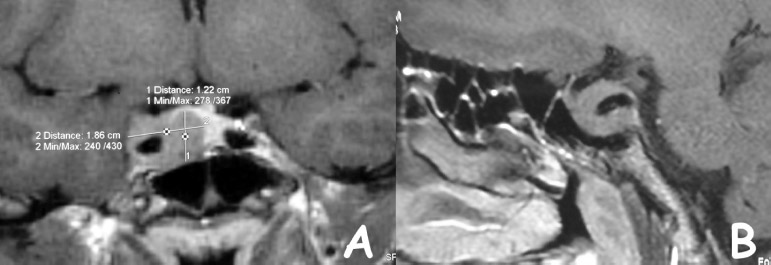
Fig. 21.4 Patient A.F. with growth hormone adenoma involving the anteroinferior and posterosuperior compartment of the right cavernous sinus (CS). The tumor displaces the lateral wall of CS laterally with subtotal encasement of the internal carotid artery. (A) An MRI coronal view clearly shows the sellar and CS components of the adenoma. (B) A sagittal view shows the involvement of the posterosuperior and anteroinferior compartments. (From Dusick Jr, et al. Avoidance of carotid artery injuries in transsphenoidal surgery with the Doppler probe and micro-hook blades. Neurosurgery 2007;60:ONS Suppl 5. Reprinted with permission. Copyright 2006 Lippincott Williams & Wilkins.)
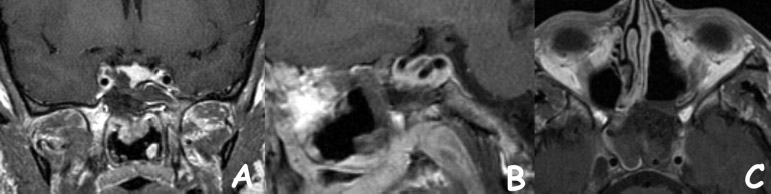
Fig. 21.5 Three-day postsurgical MRI in patient A.F. Tumor removal from the cavernous sinus (CS) (A–C) and preservation of the pituitary gland (A) are clearly visible. An axial view (C) shows the ethmoidopterygo-sphenoidal endoscopic approach with the right ethmoidectomy and middle turbinectomy and with the frontal exposition of the right CS.
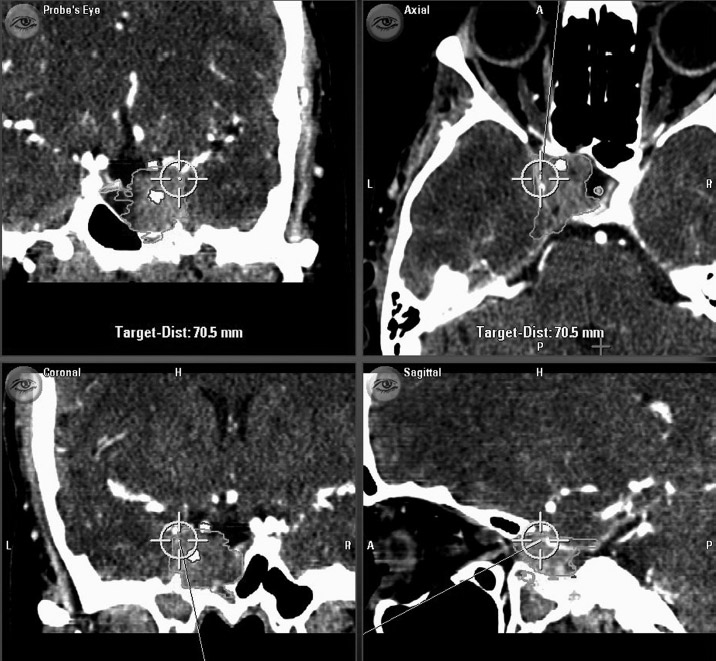
Fig. 21.6 Intraoperative computed tomography images as seen by the neuronavigator. The tumor encases the internal carotid artery (ICA) of the left cavernous sinus (CS). The pointer shows the surgical trajectory lateral to the ICA and as a tangent to the lateral wall of the CS.
In the absence of cerebrospinal fluid (CSF) leaks, the surgical cavity is simply packed with Gelfoam. If a CSF leak is detected or suspected, a multilayer plastic repair is performed by applying autologous fat in the cavity, a piece of bone or cartilage (if available) extradurally, and a mucoperiosteal flap overlay (from the middle turbinate or from the septum). It is important to remember that, to have a viable graft, it is necessary to remove the mucosa and to apply the graft directly over the bleeding surface.
The sphenoid sinus is packed with Gelfoam and, finally, the middle turbinate is medially displaced to its original position. Nasal packing is not routinely required. Lumbar drainage is not used.
Ethmoido-Pterygo-Sphenoidal Endoscopic Approach
The EPSEA is used for tumors invading the anteroinferior or lateral compartments of the CS or for tumors invading the entire CS. This procedure is the most versatile, allowing the total exposition of the CS with the possibility of simultaneous direct control of all compartments of the CS (Figs. 21.4, 21.5, and 21.6). The procedure can be schematically divided into three stages.
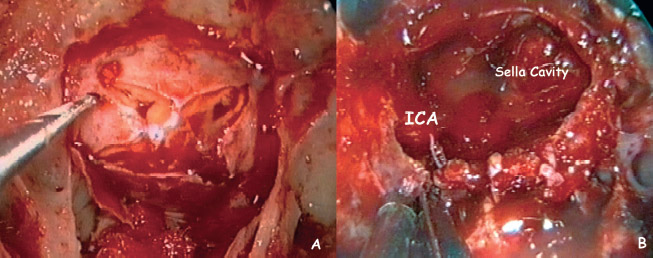
Fig. 21.7 Intraoperative view. (A) The opening of the sellar floor should be wide extending from the superior to the inferior intercavernous sinus and from one cavernous sinus (CS) to the other. (B) The bone overlying the invaded CS is removed between the opticocarotid recess to the paraclival carotid protuberance. The medial wall of the right CS in its anteroinferior portion is opened and the tumor is removed.
Stage I: Approach
An ethmoidal route is used and a complete sphenoethmoidectomy with a wide meatotomy and subtotal resection of middle turbinate is performed. The medial portion of the posterior wall of the maxillary sinus is resected to expose the posterior wall of the maxillary antrum and the vertical process of the palatine bone. After ligation of the sphenopalatine artery, the superior portion of the medial pterygoid process is drilled out. Resection of the medial pterygoid process permits the exposition of the inferolateral portion of the CS (Fig. 21.5C). A partial resection of the pterygoid process is performed, taking into account the degree of pneumatization of the lateral recess of the sphenoid and the need for visualization of the lateral and inferior walls of the sphenoid sinus.
Stage II: Opening of the Cavernous Sinus and Removal of the Tumor
To expose the anterior CS, it is necessary to remove part of the bone of the posterolateral wall of the sphenoid sinus. The bone to be removed is a quadrilateral-shaped structure located between the opticocarotid recess and the paraclival carotid protuberance medially and the orbital apex and the trigeminal nerve protuberance laterally. The vidian canal on the floor of the sphenoidal sinus is a useful landmark because it indicates the junction of the horizontal petrosal part of the carotid artery with the ascending paraclival segment of the vessel, and therefore it is a guide to the inferior portion of the CS.8
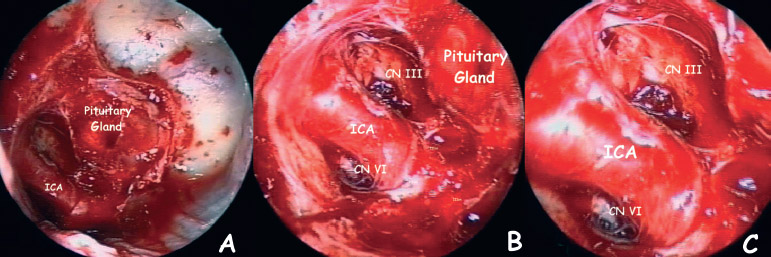
Fig. 21.8 (A–C) Intraoperative endoscopic view of the right cavernous sinus (CS) after the removal of a tumor having multifocal invasion. The medial wall of the CS is totally absent, and the internal carotid artery (ICA), the pituitary gland, and partially cranial nerves (CNs) III and VI in the lateral and anteroinferior compartments area of CS, respectively, are well visible.
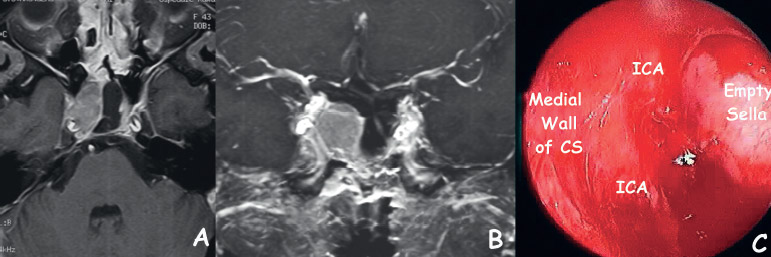
Fig. 21.9 (A–C) Recurrent nonfunctioning (NF) adenoma compressing the right cavernous sinus (CS). (A,B) Preoperative MRI: the tumor displaces posterosuperiorly the internal carotid artery, laterally to the empty sella. (C) An intraoperative view shows the integrity of the medial wall of the CS. The CS is compressed but not invaded.
The precise site of the opening of the inferior CS wall (or sphenoidal part of the medial wall) depends on the displacement that the tumor produces along the course of the carotid artery and should be performed in a safe area away from the carotid artery. When the tumor displaces the ICA medially or laterally, the incision of the wall is to be performed laterally or medially to the vessel, respectively. In cases of lesions involving the anteroinferior compartment of the CS, the ICA is generally displaced backward; in this case, the lesion covers the vessel, making the opening of the dura less dangerous. Conversely, in cases of lesions involving the posterosuperior compartment, the ICA is displaced forward and is in close contact with the anterior wall of the CS. In the latter circumstance, before any dura incision, it is mandatory to locate the position of the ICA exactly, with the combined use of neuronavigation and the micro-Doppler (Figs. 21.1, 21.2, 21.3, 21.4, 21.5, and 21.6).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


