20 Endoscope-Assisted Transsphenoidal Surgery
The direct endonasal transsphenoidal approach for removal of pituitary adenomas was described over two decades ago.1,2 Although initially a technique performed solely with the operating microscope, in recent years this approach has been increasingly performed with endoscopy either as the sole source of visualization or as providing assistance. The panoramic vision provided by the endoscope allows one to visualize and access parasellar areas not possible with the operating microscope. Effective endoscopic assistance in endonasal pituitary adenoma removal can translate into a more complete tumor removal in a widened sella, the cavernous sinus, and the suprasellar space. This chapter describes the technique of endoscopic-assisted endonasal pituitary surgery and methods of complication avoidance.
Transsphenoidal surgery emerged into the microsurgical era in the early 1970s with the advent of the operating microscope3,4 and the technique of selective adenomectomy as described by Hardy.5 Additional experience by many in the 1970s and early 1980s further improved the safety and efficacy of transsphenoidal surgery.6–14 Griffith and Veerapen2 in 1987 and Cooke and Jones1 in 1994 subsequently described the direct endonasal approach, which minimizes patient discomfort associated with the sublabial approach.1–3,15–19 This approach, which requires minimal posterior nasal mucosal dissection and no turbinate removal, is now commonly used with the operating microscope and endoscopic assistance.1,2,20–27 Advances in the technique have resulted largely from better instrumentation, surgical navigation, and, most importantly, endoscopy.28–32 The expanded visualization provided by the endoscope enables the surgeon to see into areas of the parasellar space that are not possible to see with the tunnel vision of the operating microscope. Regardless of the technique used, the surgical goal for patients with pituitary adenomas should be a selective adenomectomy with preservation or improvement of pituitary gland function. This goal is best achieved by performing a wide and tall sphenoidotomy and complete sellar bony opening to maximize sellar exposure and instrument maneuverability.33 Herein we provide a technical description of the direct endonasal approach with the operating microscope and endoscope assistance for removal of pituitary adenomas.
 Surgical Technique
Surgical Technique
Patient Preparation
Endonasal pituitary surgery is performed as originally described by Griffith and Veerapen2 with additional modifications as described below and in our recent publications.2,26,27,34,35 Preoperative antibiotics (typically cefazolin) are given and continued for 24 hours. In patients with normal preoperative adrenal function or those with Cushing’s disease, no preoperative glucocorticoids are administered.36 Those with adrenal insufficiency or borderline adrenal function are given 100 mg of intravenous hydrocortisone.
Patient Positioning and Room Setup
The endotracheal tube emerges from the left corner of the mouth, and anesthesia equipment is positioned on the left side of the patient. An arterial line and Foley catheter are placed. The patient is placed supine with the head resting freely in the horseshoe head-holder and angled approximately 30 degrees toward the left shoulder as originally described by Laws,37 which allows the surgeon to stand comfortably on the patient’s right side. The patient’s head is typically inclined in a neutral plane (0 degrees) relative to the floor for most pituitary adenomas. For lesions with marked suprasellar extension, 10 to 15 degrees of neck extension is used. The nostrils and the perinasal and right lower abdominal areas are prepped and draped in standard fashion. Topical or injected mucosal decongestants are not used.
Surgical Navigation
Surgical navigation for trajectory guidance is recommended for all endonasal transsphenoidal surgeries, unless one is highly experienced with the approach. For most patients with a pituitary adenoma, C-arm fluoroscopy is simple and effective for giving excellent trajectory guidance in the sagittal plane. Frameless stereotactic surgical navigation based on either a preoperative magnetic resonance imaging (MRI) or computed tomography (CT) scan provides significantly more data than fluoroscopy. It is particularly helpful in patients with prior surgery or large invasive tumors with markedly distorted anatomical landmarks. If fluoroscopy is used, the base of the operating microscope is placed just outside the arc of the C-arm above the patient’s head, with the microscope to the patient’s right side.
Endoscopic Equipment and Setup
The endoscope video monitor and tower are placed above the patient’s head on the patient’s left side to allow for comfortable viewing by the surgeon and the assistant who will be standing on the patient’s right side. Standard 4-mm rigid endoscopes (18 cm long) with 0-, 30-, and 45-degree angled lenses should be available. An endoscope holder, which is often helpful, can also be positioned with the insertion device fixed to the leftmost cephalad aspect of the operating table.
Surgical Instrumentation
Given the narrow working space of the endonasal approach, all instruments should be as low profile as possible with angled or bayoneted handles to minimize visual obstruction and to maximize instrument maneuverability. For example, Cottle dissectors, microdissectors, ring curettes, and microblades are on bayoneted handles, whereas microscissors and tumor forceps are of a single-shaft pistol-grip construction to minimize visual obstruction. High-speed drills and ultrasonic aspirators are also of the lowest possible diameter with angled hand-pieces. A micro-Doppler probe is also used for all cases to localize the cavernous carotid arteries prior to dural opening.29 Short (60- to 70-mm) endonasal speculums also enhance maneuverability and increase exposure compared with longer speculums as shown in Fig. 20.1.30
Nasal Approach and Sphenoidotomy
The initial portion of the procedure is performed with the operating microscope and a handheld speculum. The nostril chosen for the approach is based largely on tumor location as defined by the patient’s preoperative MRI. For tumors projecting more to one side of the sella, the contralateral nostril is used, given that exposure across the midline to the contralateral sella and cavernous sinus (CS) area is consistently wider than to the ipsilateral side. This rule also applies in the great majority of patients with septal deviations. In patients with relatively midline tumors, the right nostril is used, given that the surgeon stands on the patient’s right side, and this affords a more comfortable operating position. A relaxing alar incision, although used occasionally early in our experience to accommodate the endonasal speculum, has not been used in more than 550 cases given the availability of smaller and thinner speculums.
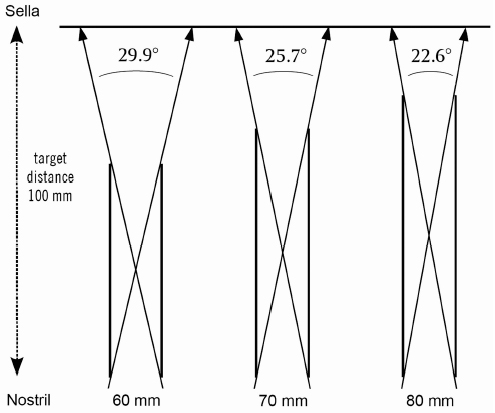
Fig. 20.1 Line drawings comparing the 60-mm, 70-mm, and 80-mm speculums depicted as parallel lines with 16 mm proximal and distal openings and a target distance of 100 mm from the nostril to the sellar target. Note the increase in the angle of exposure for the 60-mm speculum. The width of exposure at the 100-mm target is 37 mm for the 60-mm speculum compared with 30 mm for the 70-mm speculum and 24 mm for the 80-mm speculum. (From Fatemi N, Dusick JR, Malkasian D, et al. Instrumentation assessment: short trapezoidal speculums for suprasellar and infrasellar exposure in endonasal trans-sphenoidal surgery. Neurosurgery 2008;62(5 Suppl 2):ONS325–329; discussion ONS329–330. Reprinted with permission.)
The handheld speculum is passed into the anterior nostril to identify the inferior and middle turbinates. The speculum is then gently passed along the trajectory of the middle turbinate with care being taken to minimize trauma to the anterior and midnasal septum and turbinates. The speculum blades gently displace the middle turbinate laterally and pass further into the nasal cavity to expose the junction of the keel of the sphenoid and the posterior nasal septum. After confirming the correct trajectory to the sella with fluoroscopy or surgical navigation, the posterior septal mucosa is cauterized with a bipolar cautery in a vertical swath, and a vertical mucosal incision of approximately 2 cm is made with a Cottle elevator. The mucosa is reflected laterally to expose the midline sphenoid keel and ipsilateral sphenoid ostium, which is typically superolateral to the equator of the keel at the 10 o’clock or 2 o’clock positions. The posterior nasal septum is then displaced off the midline by the distal tips of the handheld speculum to allow exposure of the contralateral side of the keel and the contralateral ostium. The Cottle elevator can also be used to further reflect this contralateral mucosa.
After the sphenoid keel and ostia are exposed, the handheld speculum is replaced by a self-retaining endonasal speculum, typically 60 to 70 mm long (Mizuho America, Beverly, MA).30 The distal speculum blades should straddle the sphenoid keel, with the ostia visualized bilaterally, and the nasal end of the speculum should be flush with the nostril. If the ostia are seen higher than the 10 o’clock and 2 o’clock positions, the speculum trajectory is likely to be too far inferior and should be re-angled more superiorly and confirmed with fluoroscopy or surgical navigation. The added exposure from the use of a shorter speculum is shown in Fig. 20.1.
A wide and tall sphenoidotomy is next performed with pituitary and Kerrison rongeurs. Sphenoid bone and mucosal removal should extend beyond the lateral edges of the ostia bilaterally and allow visualization of the tuberculum sella and sellar floor. To maximize maneuverability of instruments during the endoscopic phase of the procedure (described below), removing bone up close to the ethmoid roof and down to a level flush with the floor of the sphenoid sinus is recommended. As we have recently shown, a smaller and less complete sphenoidotomy will otherwise restrict maneuverability and visualization and has been associated with incomplete tumor removal (Fig. 20.2).33
Because the sphenopalatine arteries run in the posterior inferior nasal mucosa at approximately the 8 o’clock and 4 o’clock positions, it is best to displace this mucosa laterally with the speculum or to cauterize it prior to removing it to avoid injuring the vessels with the rongeurs. This bleeding, however, can be stopped relatively easily with bipolar or monopolar cautery.
Sellar Bony Opening and Carotid Localization
After the sphenoidotomy, the sellar face is identified and the operative view of intrasphenoidal bony septations should be correlated with those septations seen on the patient’s preoperative MRI. Septations ending on the sellar face are removed with a rongeur down to the sella; those that end over a carotid artery should be removed with care, and excessive torquing of the bone fragments should be avoided. Mucosa over the sella is removed, but sphenoid sinus mucosa in the lateral aspects and roof of the sphenoid sinus can be left undisturbed. The sellar bone is then removed from CS to CS and from the sellar floor inferiorly to the tuberculum sella superiorly with a Kerrison rongeur or in some instances with a high-speed diamond bit drill. In patients with large invasive tumors, the sellar bone may be markedly thinned or absent and tumor may be directly under the mucosa or under an attenuated or absent sellar dura.
After the sellar bone removal and before dural opening, a micro-Doppler probe is used to localize the cavernous carotid arteries (10-MHz ES-100X MiniDop with NRP-10H bayonet probe [Koven, St. Louis, MO] or 20-MHz Surgical Doppler [Mizuho America]). As previously described and shown in Fig. 20.3, the probe is placed initially at the edge of the bony opening at 90 degrees to the dura.29 If only faint or no audible flow is present, the probe is angled more laterally under the bone edge. In most patients, this angulation results in the carotid flow becoming louder. The probe is then moved superiorly and inferiorly to further determine the carotid course. Typically, the carotids have their most medial course superiorly near the tuberculum sella just before they pass through the dural ring to enter the subarachnoid space. If no flow is evident, then additional bone can be removed laterally to enlarge sellar exposure. If audible flow is still absent, consideration should be given to whether the probe is malfunctioning, which can occur on occasion.
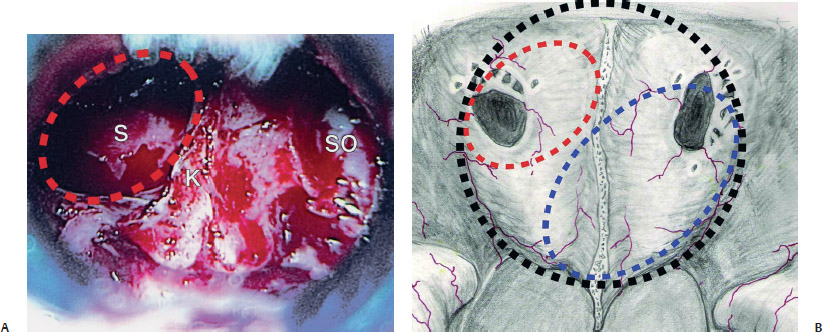
Fig. 20.2 (A) Intraoperative photograph of the sphenoid keel in a patient with prior endonasal surgery showing that at the original surgery, only bone to the right of the keel had been removed, whereas the midline keel and left half of sphenoid bone and sphenoid ostium were left intact. K, sphenoid keel; S, prior opening into sphenoid sinus; SO, sphenoid ostium. (B) Drawing of variations on the restricted sphenoid keel openings seen at reoperation shown as shaded circles and ovals. The red oval represents the extent of bone removal in the patient in A, whereas the blue oval
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


