Purpose
To compare the effectiveness of pars plana vitrectomy endoresection with iodine-125 brachytherapy in the treatment of choroidal melanoma.
Design
A nested case-control study (1:2) from a surgical cohort.
Methods
The study comprised 81 choroidal melanoma patients treated with either endoresection or iodine-125 brachytherapy. Twenty-seven patients who had undergone endoresection were matched according to tumor height and postequatorial tumor location with 54 cases treated with iodine-125 brachytherapy. Metastatic disease, overall survival, local tumor recurrence, visual acuity, and secondary enucleation rates were analyzed and compared between groups.
Results
Metastatic spread was observed in 11 patients in the iodine-125 brachytherapy group vs only 1 patient in the endoresection group (20.4% and 3.7%, respectively, P = .053). Fourteen patients died during follow-up: 11 in the brachytherapy arm vs 3 in the endoresection arm (20.4% and 11.1%, respectively, P = .238). For the iodine-125 brachytherapy and endoresection groups, respectively, the 5-year Kaplan-Meier estimates were as follows: overall survival, 81.5% vs 89.2% (log-rank test, P = .429;); relapse-free survival, 96.6% vs 92.4% ( P = .2); visual acuity retention equal or superior to 20/200, 66.4% vs 59.9% ( P = .083), and eye retention, 85.7% vs 87.8% ( P = .942).
Conclusions
Endoresection for choroidal melanoma is an effective treatment modality in selected cases of posterior choroidal melanomas, with outcomes similar to those obtained with iodine-125 brachytherapy.
The treatment of posterior choroidal melanoma remains challenging and the optimal approach is still unclear. Most treatments are eye-preserving techniques such as transpupillary thermotherapy, plaque brachytherapy, proton-beam radiotherapy, trans-scleral tumor resection, and endoresection. The most widely used conservative treatment for uveal melanoma is iodine-125 brachytherapy. The local tumor recurrence rate after iodine-125 brachytherapy can be as low as 10%, with eye retention in approximately 80% of patients, even in the case of large tumors.
Peyman and associates were among the first authors to describe an alternative conservative approach in which internal resection is performed via the pars plana using vitrectomy instruments. Later, Damato and associates treated 52 uveal melanoma patients using this same internal approach, which they termed “endoresection.” García-Arumi and associates reported the long-term outcomes of this technique in a group of patients treated for high posterior choroidal melanoma.
Pars plana vitrectomy endoresection has been described as a primary procedure for tumors in patients who are not expected to have good outcomes after more conventional forms of treatment or as a secondary procedure used after toxic tumor syndrome. Some authors advocate the use of neoadjuvant proton beam or stereotactic radiotherapy before endoresection. Whether used alone or with adjuvant radiotherapy, endoresection appears to be a reasonable approach to a rapidly growing melanoma located in the posterior pole, especially when the tumor exhibits pronounced height and a small base diameter. Some authors consider endoresection to be preferable in these cases because of the large tumor size, the added morbidity associated with the proximity of the tumor to the optic disc/fovea, and the difficulty of treating these tumors with radiotherapy modalities. However, endoresection remains a highly controversial technique because of the theoretical risk of tumor dissemination when using this approach, although such concerns have been voiced for radiotherapy and enucleation as well.
The aim of this study was to compare endoresection to iodine-125 brachytherapy in patients with uveal melanomas limited to the equatorial area. We report the comparative results in terms of metastatic disease, overall patient survival, local tumor recurrence, visual function, and eye retention.
Patients and Methods
This was a nested case-control study (1:2) based on a historical surgical cohort. From September 1995 through May 2010, 416 patients diagnosed with uveal melanoma were treated at the Ocular Oncology Unit of the Ophthalmology Department of Bellvitge University Hospital and at the Brachytherapy Department of the Catalan Oncology Institute. We selected 27 consecutive patients who had undergone endoresection and matched them according to tumor height and postequatorial tumor location with 54 patients who had been treated with iodine-125 brachytherapy. Patient confidentiality was protected by national data confidentiality laws. This manuscript has been revised for publication by the Clinical Research Ethics Committee of Bellvitge University Hospital (IRB00005523). Written informed consent was obtained from all subjects in accordance with our institutional guidelines. This study adhered to the tenets of the Declaration of Helsinki.
All patients included in the study presented uveal melanomas located close to the optic nerve and/or fovea. In all cases, the anterior margins did not extend beyond the equator of the eye. None of the patients had scleral involvement or evidence of distant metastasis at the time of study inclusion. The tumor characteristics for both groups are presented in Tables 1 and 2 .
| Brachytherapy (n = 54) Median (IQR) | Endoresection (n = 27) Median (IQR) | P Value b | |
|---|---|---|---|
| Age (y) a | 55.99 (14.66) | 64.05 (15.05) | .027 |
| Visual acuity (Snellen chart) | 0.5 (0.7) | 0.2 (0.5) | .084 |
| Visual acuity (logMAR) | 0.301 (0.903) | 0.699 (2.78) | .084 |
| Height (mm) a | 6.95 (1.8) | 7.69 (2.27) | .117 |
| Tumor horizontal base (mm) | 12.0 (3.0) | 10.0 (3.0) | <.001 |
| Tumor vertical base (mm) | 12.0 (2.5) | 10.0 (4.0) | .020 |
| Tumor maximum diameter base (mm) | 12.5 (2.0) | 11.0 (2.9) | <.001 |
| Fovea distance (mm) a | 5.22 (3.52) | 3.33 (2.93) | .020 |
| Optic nerve distance (mm) a | 5.49 (3.31) | 2.80 (2.99) | .001 |
a Normal distribution, mean (SD).
b P values were obtained by Mann-Whitney U test or Student t test as needed.
| Brachytherapy (n = 54) | Endoresection (n = 27) | P Value c | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Sex | |||||
| Men | 27 | 50.0 | 13 | 48.1 | .875 |
| Women | 27 | 50.0 | 14 | 51.9 | |
| Eye | |||||
| Right | 29 | 53.7 | 14 | 51.9 | .672 |
| Left | 22 | 40.7 | 13 | 48.1 | |
| Tumor size a | |||||
| Medium | 50 | 92.6 | 22 | 81.5 | .152 |
| Large | 4 | 7.4 | 5 | 18.5 | |
| Tumor size b | |||||
| T1 | 1 | 1.9 | 1 | 3.7 | .149 |
| T2 | 26 | 48.1 | 17 | 63.0 | |
| T3 | 27 | 50.0 | 9 | 33.3 | |
| Retinal detachment | |||||
| No | 24 | 44.4 | 6 | 22.2 | .051 |
| Yes | 30 | 55.6 | 21 | 77.8 | |
| Visual acuity | |||||
| 20/200 or better | 42 | 77.8 | 18 | 66.7 | .058 |
| Inferior to 20/200 | 12 | 22.2 | 9 | 33.3 | |
| Bruch membrane rupture | |||||
| No | 33 | 61.1 | 3 | 11.1 | <.001 |
| Yes | 21 | 38.9 | 24 | 88.9 | |
a According to COMS classification.
b According to the 7th edition of AJCC staging.
c P values were obtained by χ 2 or Fisher exact test as needed.
Treatment and Follow-up
Patients were fully informed of all relevant aspects of the procedures, including the controversy surrounding endoresection. The preoperative examination included a best-corrected Snellen visual acuity test, a complete ophthalmoscopic examination, and A- and B-scans to measure the maximum tumor thickness and diameter. Tumor size was classified according to the criteria established by the Collaborative Ocular Melanoma Study (COMS) and according to the tumor size categories (T) published in the 7th edition of the American Joint Committee of Cancer (AJCC) staging system. All patients underwent screening for metastatic disease, which included serum biochemistry with liver function determinations, ultrasound evaluation of the liver, chest radiography, and evaluation by an oncologist.
Brachytherapy was administered using iodine-125 COMS-type plaques. Trans-scleral illumination was used to assess tumor margins with the patient under local anesthesia. In all cases, a minimum safety margin of 2 mm was employed and the same surgeon (J.M.C.) performed all procedures in the Brachytherapy Department. A total dose of 85 Gy was delivered to the apex of the tumor using a dose rate of 50-120 cGy/hour. Initial follow-up was performed approximately 15 days after the intervention and at 3 months; thereafter, follow-up assessment, including screening for metastasis, was performed every 6 months during the first 5 years and annually thereafter.
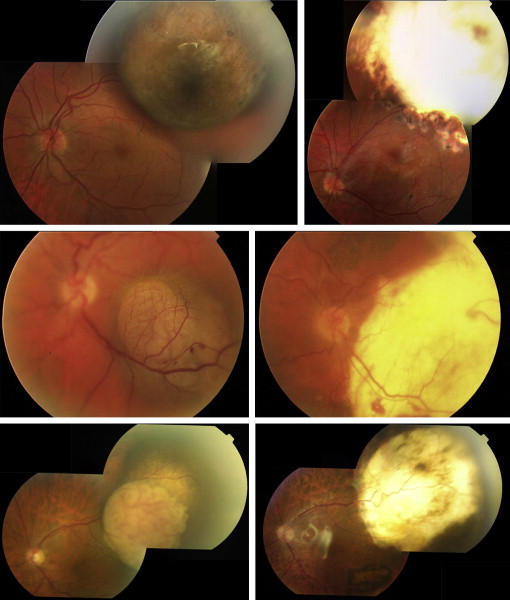
In the case of endoresection, the surgical technique varied according to the degree of tumor invasion. In cases where the tumor had not invaded the retina, endoresection consisted of 20- to 23-gauge vitrectomy using a panoramic viewing system, followed by posterior hyaloid dissection, large retinotomy anterior to the tumor, and laser endophotocoagulation with 600-800 mW directed 2 mm beyond the tumor margins using the continuous mode of a 532-nm laser. The melanoma lesion was removed with the vitrectomy probe using a bimanual technique to separate and protect the retina. Intraoperative choroidal bleeding was controlled by temporarily raising the intraocular pressure (IOP) to 60-70 mm. In all cases, patient blood pressure remained within normal limits during the procedure. Tumor excision was performed from the tumor apex to the scleral bed. Cellular remnants at the scleral bed were photocoagulated with high doses (800-1000 mW) of continuous-mode laser endophotocoagulation at 532 nm. The retina was reattached with perfluorocarbon liquid. Laser retinopexy endophotocoagulation was performed at the margins of the retinotomy, and this procedure was followed by fluid-air exchange and silicone oil-air exchange (1300-5000 centistokes). In cases where the tumor had invaded the retina, continuous-mode laser endophotocoagulation at 532 nm was employed through the retina and around the tumor margins, and then both the tumor and the retina were removed without peripheral retinotomy. In all cases, the lens of the eye was removed before vitrectomy by phacoemulsification, and a 3-piece foldable acrylic intraocular lens was inserted. Patients were instructed to maintain a face-down position for 1 week after surgery. Postoperative follow-up was performed at 1 day, 1 week, 1 month, 3 months, and 6 months. Thereafter, follow-up, including screening for metastasis, was performed at 6-month intervals ( Figure 1 ).
Statistics
Descriptive analysis was performed, and measures of the central value (mean and median) and dispersion (standard deviation, interquartile range) were determined depending on whether there was a normal distribution (Kolmogorov-Smirnov test). For quantitative variables, the Student t test or the Mann-Whitney U test was used, as appropriate, to compare baseline characteristics resulting from tumor endoresection or iodine-125 brachytherapy. To evaluate differences in proportions, the χ 2 test or Fisher exact test was employed as needed.
A Kaplan-Meier analysis was performed to determine predictive variables of overall survival. Those variables that showed a statistically significant association with survival by the log-rank test ( P < .05) were subsequently analyzed using a Cox regression model. Effect estimates were expressed as hazard ratios (HR) with 95% confidence intervals (95% CI). All statistical tests were 2-tailed, and P values of ≤.05 were deemed significant. All analyses were performed using SPSS 12.0 software (SPSS, Inc, Chicago, Illinois, USA).
Results
A total of 81 patients (54 treated by iodine-125 brachytherapy and 27 with endoresection) were evaluated. Patients in the iodine-125 brachytherapy and endoresection groups presented with comparable tumor heights and locations (posterior) and were comparable in terms of sex, eye affected, follow-up, and tumor size according to the COMS criteria and the T categories of the 7th edition of the AJCC staging system. Most tumors in both groups were classified as medium-sized (92.6% of the iodine-125 brachytherapy group and 81.5% of the endoresection group; P = .152) and as T2 or T3 (98% of the iodine-125 brachytherapy group and 96% of the endoresection group; P = .149). The mean follow-up period was 59.37 ± 33.64 months (range, 12-138 months) for the endoresection group and 70.52 ± 37.15 months (range, 12-148 months) for the iodine-125 brachytherapy group ( Tables 1-3 ).
| Brachytherapy (n = 54) | Endoresection (n = 27) | P Value a | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Metastatic disease | |||||
| No | 43 | 79.6 | 26 | 96.3 | .053 |
| Yes | 11 | 20.4 | 1 | 3.7 | |
| Observed death | |||||
| No | 43 | 79.6 | 24 | 88.9 | .238 |
| Yes | 11 | 20.4 | 3 | 11.1 | |
| Specific death | |||||
| No | 44 | 81.5 | 26 | 96.3 | .089 |
| Yes | 10 | 18.5 | 1 | 3.7 | |
| Local recurrence | |||||
| No | 53 | 98.2 | 25 | 92.6 | .256 |
| Yes | 1 | 1.8 | 2 | 7.4 | |
| Enucleation | |||||
| No | 47 | 87.0 | 24 | 88.9 | ≥.999 |
| Yes | 7 | 13.0 | 3 | 11.1 | |
| Enucleation cause | |||||
| Retinal detachment | 1 | 1.9 | 0 | 0 | .057 |
| Neovascular glaucoma | 5 | 9.3 | 0 | 0 | |
| Phthisis bulbi | 0 | 0 | 1 | 3.7 | |
| Local recurrence | 1 | 1.9 | 2 | 7.4 | |
| Enucleation cause | |||||
| Complication | 6 | 11.1 | 1 | 3.7 | .183 |
| Local recurrence | 1 | 1.9 | 2 | 7.4 | |
| Final VA | |||||
| Inferior of 20/200 | 35 | 64.8 | 21 | 77.8 | .234 |
| 20/200 or better | 19 | 35.2 | 6 | 22.2 | |
| Final VA (logMAR) | |||||
| Median (IQR) | 2.01 | (1.17) | 2.56 | (0.83) | .234 |
| Follow-up (mo) | |||||
| Median (IQR) | 70.52 | (37.15) | 59.37 | (33.64) | .193 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


