Chapter 14 Endophthalmitis
Exogenous bacterial endophthalmitis
Cataract surgery
Exogenous endophthalmitis in adults occurs most frequently following intraocular surgery (70−80%). Cataract extraction has a reported incidence of postoperative endophthalmitis of 0.1−0.38%1 (Fig. 14.1). Good et al. reported an incidence of 0.45% in a retrospective review of 641 cases of cataract extraction in children.2 Wheeler et al. reported an incidence of 0.07% in children undergoing cataract and glaucoma surgery.3
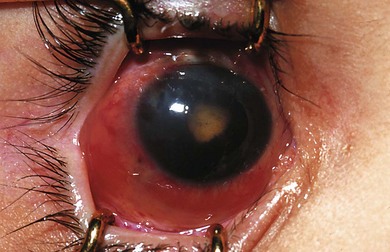
Fig. 14.1 Bacterial endophthalmitis following infant cataract surgery and intraocular lens implantation.
The Endophthalmitis Vitrectomy Study (EVS) studied 420 cases of infectious endophthalmitis presenting within 6 weeks of cataract extraction or secondary intraocular lens implantation.4 Positive culture was obtained from 69.3% of intraocular specimens. Gram-positive bacteria were isolated in 94.2% of cases and Gram-negative bacteria in 6.5% of isolates. Staphylococcus epidermidis, normal skin flora, was by far the most common gram-positive isolate (70%), followed by Staphylococcus aureus (9.9%), Streptococcus spp. (2.2%), and Propionibacterium acnes. Proteus and Pseudomonas were the most common Gram-negative organisms. Haemophilus influenzae has also been identified in other series.5 Weinstein’s study of children with endophthalmitis reported similar results, 75% of culture positive cases being caused by Gram-positive organisms.6 Staphylococcus epidermidis, Streptococcus pneumoniae, and Staphylococcus aureus have been identified as the most frequent infecting agents in children following cataract extraction.
Trauma
Trauma is a significant cause of exogenous endophthalmitis in children. Endophthalmitis following penetrating injury accounted for 44% of cases in a 10-year review of pediatric endophthalmitis.7 The incidence of endophthalmitis after penetrating injury ranges from 4% to 20% and is particularly high when injury occurs in a rural setting.8 Eight-five percent of patients in the Endophthalmitis Vitrectomy Study (EVS) achieved final visual acuity of 20/400 or better while only 22−42% achieved this level of acuity following post-traumatic endophthalmitis.4,9
Glaucoma filtration surgery
Infection associated with filtration surgery is often sub-classified into blebitis, defined as mucopurulent material in and around the bleb associated with anterior segment activity but without hypopyon. If a hypopyon is present, or there is evidence of vitreous activity, a diagnosis of endophthalmitis is made. Endophthalmitis may occur soon after surgery, but is frequently reported many years after surgery. Antimetabolites such as 5-fluorouracil (5-FU) and mitomycin C are used to augment filtration surgery in childhood glaucoma. While improving the success rate of filtration surgery they increase the risk of postoperative endophthalmitis. When intraoperative 5-FU is used, the reported incidence of endophthalmitis is 1−5.7%. The incidence of endophthalmitis is 0.3−4.9% when mitomycin C is applied.10
Implantation of glaucoma drainage devices is associated with increased rates of endophthalmitis. A review of 542 eyes with Ahmed valve insertion noted an endophthalmitis rate significantly higher in children. The incidence in adults was 1.7%, compared to 4.4% in children.11 Endophthalmitis is often associated with conjunctival erosion and tube exposure; inferior placement of bleb or drainage device is also associated with higher rates of infection. When endophthalmitis is related to glaucoma surgery, the spectrum of microorganisms differs from that in cataract surgery in that streptococcal species predominate. Haemophilus influenzae is also isolated more frequently than Staphylococcus epidermidis. This difference may reflect the fact that endophthalmitis is often of late onset with invasion of microorganisms through thin walled or leaking blebs.12 Jampel et al. found increased incidence of endophthalmitis associated with full thickness filtration procedures, inferior placed blebs, bleb leakage, and the use of mitomycin.13 If endophthalmitis develops in the early postoperative period, Staphylococcus epidermidis is more frequently cultured.
Strabismus surgery
Endophthalmitis following strabismus surgery is rare, with an incidence of 1 : 3500 to 1 : 185 000.14 Scleral perforation is thought to be a prerequisite for the development of endophthalmitis following strabismus surgery. Spatulated needles have greatly reduced the frequency of scleral perforation during strabismus surgery. Needles and sutures are frequently contaminated despite the use of preoperative povidone-iodine. Carothers et al. noted 19% of needles and 24% of sutures were culture positive in patients undergoing strabismus surgery.15
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


