Chapter 5 Emmetropization, refraction and refractive errors
control of postnatal eye growth, current and developing treatments
Refractive error is the most common eye disorder, affecting over a third of adults, and is the cause of a significant burden of visual impairment in the world. The prevalence varies widely among countries; myopia is associated with education, urbanization, and affluence. The prevalence of myopia varies between 7% and 70% depending on the age, occupation, and educational status of those studied.1 In some East Asian countries, myopia is becoming more common; indeed, it has reached epidemic proportions with over 80% of school leavers and up to 50% of 9-year-olds being myopic.2 Myopia prevalence is increasing in developed countries with an approximate 1 diopter myopic shift in the US population between 1971 and 1999–2004.3 The blinding complications of myopia (myopic retinal degeneration, retinal detachment, glaucoma, cataract) occur in highly myopic eyes (pathological myopia). The younger the onset, the faster the rate of progression and the higher the end myopic results. UK data suggests children myopic before the age of 9 years are likely to be at least 6 diopters myopic by adulthood.4
Postnatal growth and emmetropization
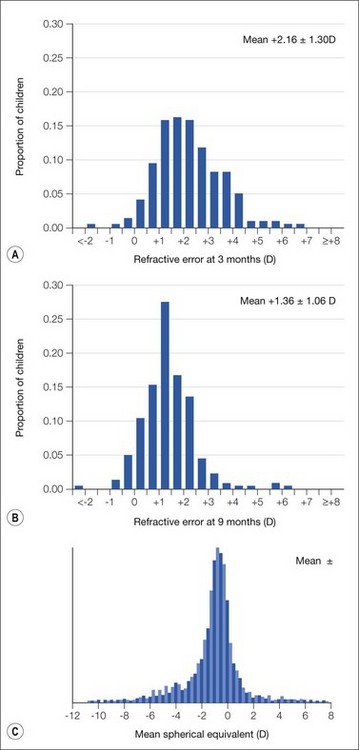
Refractive error is a mismatch between the optical refractive determinants of the eye (corneal curvature, lens power and location, and axial length). At birth, the eye is rarely emmetropic, and is significantly smaller than the adult eye (Table 5.1); the refractive error of the newborn eye ranges between +2.0 and +4.0 diopters (D) with an almost normal (Gaussian) distribution (Fig. 5.1A).5 Within 2 years, this variability of refractive error decreases and the mean value shifts so that the eye becomes closer to emmetropia. The population distribution becomes more leptokurtotic, which means it is more clustered around the mean value (Fig. 5.1B). This process is called emmetropization and, within populations, it is possible to predict shifts in refractive error so that most of the infants born hyperopic become emmetropic by 6 to 8 years of age. Eye growth is rapid, and reaches 90% of adult proportions by the age of 4. As the cornea flattens, it loses refractive power, which is balanced by increasing axial length. Whether this balance is guided by genetically encoded mechanisms or is affected by environmental influences has been debated for centuries. Most likely both nature and nurture affect the way the eye develops. By adulthood, the distribution of refractive error is similarly leptokurtotic, and there is a left skew in the distribution of the myopic subjects (Fig. 5.1C).6
Table 5.1 Newborn vs. adult ocular parameters
| Newborn | Adult | |
|---|---|---|
| Axial length | 16.8 mm | 23.0 mm |
| Mean keratometry | 55 D | 43 D |
| Optic nerve length | 24 mm | 30 mm |
| Corneal diameter | 10 mm | 10.6 mm (vertical) × 11.7 mm (horiz.) |
| Corneal thickness | 581 µm | 545 µm |
| Pars plana length | 0.5–1.05 mm | 3.5–4 mm |
| Orbital volume | 7 cc | 30 cc |
Support for the assertion that eye growth is genetically regulated comes from studies of heritability and epidemiology. Almost all studies of refractive error, and in particular myopia, have shown that the strongest risk factors are having one or two parents who are myopic,7 and pediatric ophthalmologists recognize the hyperopic/esotropic family attending their practices. While this might be ascribed to families sharing the same environmental risk factors, twin studies control for this shared environment by comparing concordance between monozygotic (identical) and dizygotic (fraternal) twin pairs. Twin studies, across ages and cultures, show a high heritability of refractive error, of the order of 80–90%.8,9 This is not to say that the environment is not important. Strong temporal trends in myopia prevalence must be due to environmental factors. However, genetic factors appear important in determining where a person lies within the population distribution of a society at a particular time. Recently, genome-wide association studies have reported the association of several genes with refractive error,10,11 and further genes will be identified. Like many complex traits, myopia susceptibility is conferred by many genes of small effect.
There is a significant association of myopia with near work, educational level of attainment, and IQ.12 The classic study by Zylbermann et al.13
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


