Purpose
Previous studies suggest that hormone therapy favorably affects intraocular pressure (IOP). Here, we examined the association between hormone therapy use and IOP in the context of a large randomized trial.
Design
Secondary data analysis from a randomized controlled trial.
Methods
We used data from the Women’s Health Initiative-Sight Exam (WHISE). Women with prior hysterectomy received oral conjugated equine estrogen (0.625 mg/day) or placebo. Women with a uterus received estrogen plus progestin (medroxyprogesterone acetate 2.5 mg/day) or placebo. IOP was measured 5 years after randomization. Adjusted linear regression models were used to assess the association between hormone therapy and IOP.
Results
The WHISE included 1668 women in the estrogen-alone trial (aged 63–86, mean 72 years) and 2679 women in the estrogen-plus-progestin trial (aged 63–87, mean 72 years). In multivariate analyses, compared to placebo treatment, treatment with estrogen alone was associated with a 0.5 mm Hg reduction of the IOP in the right eye (95% CI: −0.8, −0.1, P = .005) and a 0.6 mm Hg (95% CI: −0.9, −0.3, P < .001) reduction of the IOP in the left eye. In the estrogen-plus-progestin trial, there was no significant difference in IOP between the treatment and placebo groups ( P = .30 right eye and P = .43 left eye).
Conclusions
This study represents an IOP analysis in the largest hormone trial available. Estrogen-alone therapy in postmenopausal women is associated with a small but significant IOP reduction of 0.5 mm Hg. The clinical significance of this small decrease remains to be determined.
Glaucoma is the leading cause of irreversible blindness worldwide, and the global burden is increasing as the population ages. Based on a recent meta-analysis of 50 population-based studies, glaucoma was estimated to affect 64.3 million people aged 40–80 years in 2013, and that number is predicted to increase to 76 million in 2020 and to 111.8 million in 2040. Women comprise the majority of glaucoma cases worldwide and in the United States (U.S.). In certain regions, women have less access to eye care than do men; even in developed nations such as the U.S., women are 24% less likely than are men to receive treatment for glaucoma. Primary open-angle glaucoma (POAG) is the most common type of glaucoma in the U.S., and although a recent meta-analysis suggested that men have a 36% greater risk of POAG than do women, women comprise the majority of POAG cases in the U.S., perhaps as a result of their longer lifespans. At present, POAG affects 1.44 million women in the U.S., and that number is projected to increase to 3.66 million by 2050. Thus, from a public health perspective, glaucoma screening and prevention in women is vital.
The risk of POAG in women is affected not only by chronological age but also by advancing reproductive age. For example, in a Mayo Clinic study of 1044 women, early menopause as a result of bilateral oophorectomy before the age of 43 years was associated with a 1.6-fold increase in the risk for POAG. Menopausal stage and sex steroid hormones influence the level of intraocular pressure (IOP), the major risk factor for glaucoma, and is the only one that is modifiable. The Early Manifest Glaucoma Treatment Trial (EMGT) suggested that each 1 mm Hg reduction in IOP decreases the risk of glaucoma progression by 10% in patients with early POAG, normal-tension glaucoma, and exfoliation glaucoma. Compared to age-matched premenopausal women, postmenopausal women exhibited 1.5–2 mm Hg greater IOP. Small randomized trials and observational studies have shown that IOP decreased by 1–5 mm Hg following treatment with hormone therapy in postmenopausal women with and without POAG. Based on these findings and those of the EMGT, the observed IOP reduction, though small in magnitude, may be clinically significant in postmenopausal women with glaucoma.
Notably, prior studies also suggest that medroxyprogesterone acetate can minimize the beneficial effects of estrogen in the central nervous system. Similarly, a large claims database of 152 163 enrollees aged >50 years showed that each additional month of hormone therapy containing estrogen, but not a combination of estrogen and progesterone, was associated with a 0.4% reduced risk for POAG.
To date, however, there has been no large, randomized, placebo-controlled trial with longitudinal follow-up designed to assess the effect of postmenopausal hormone therapy on IOP. To examine the effect of estrogen and estrogen plus progestin on IOP in the context of a large randomized clinical trial, we performed a secondary data analysis of IOP outcomes on data collected during the Women’s Health Initiative Sight Exam (WHISE) study, an ancillary study of the Women’s Health Initiative (WHI) randomized hormone trial that focused on age-related macular degeneration (AMD). IOP was measured 5 years after baseline in 2 groups: (1) women with prior hysterectomy who were randomized to receive either conjugated equine estrogens (estrogen-alone trial) or placebo; and (2) women with a uterus who were randomized to receive conjugated equine estrogens combined with medroxyprogesterone acetate (estrogen-plus-progestin trial) or placebo. Based on previous findings, we hypothesized that women who had been randomized to receive conjugated equine estrogens would have lower IOP compared to women randomized to receive placebo. In contrast, we hypothesized that this association would not be observed in women randomized to receive conjugated equine estrogens and medroxyprogesterone acetate.
Methods
Study Design and Population
The WHI (the parent study) was a 15-year research program initiated in 1991 by the National Institutes of Health consisting of a set of clinical trials and an observational study, which together involved 161 808 generally healthy postmenopausal women aged 50–79 years. The clinical trials were designed to test the effects of hormone therapy, diet modification, and calcium and vitamin D supplementation on the incidence of heart disease, fractures, and breast and colorectal cancer. The hormone trial was stratified by hysterectomy status: the estrogen-plus-progestin study of women with a uterus and the estrogen-alone study of women without a uterus (ie, those who had undergone hysterectomy). Of note, women with a uterus received progestin in combination with estrogen, a practice known to prevent endometrial cancer. Within each stratum, the women were randomly assigned to either a hormone or a placebo arm. The WHI trial has been registered at clinicaltrials.gov (identifier is NCT00000611 ).
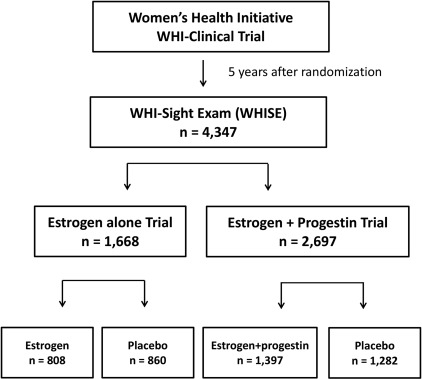
The present study was a secondary analysis of IOP data from the WHISE, an ancillary study to the WHI randomized hormone therapy trial. The WHISE study was conducted between 2000 and 2002 to examine the association between prior randomization to hormone therapy and AMD, where early or late AMD was assessed based on fundus photography in women 65 years and older an average of 5 years after randomization to hormone therapy or placebo. WHISE recruited 4347 women who underwent fundus photography of at least 1 eye at 21 WHI clinics. A flow diagram of the WHISE study is presented in the Figure . Overall, the WHISE study reached 96.6% of its enrollment goal of 4500 eligible and consenting participants (15.9% of the WHI hormone trial, n = 27 347) before termination of the estrogen plus progestin study arm owing to an adverse risk-benefit profile after an average follow-up period of 5.2 years. The WHISE protocol was approved by Institutional Review Boards at each clinic site, and all participants provided written informed consent to participate. The Institutional Review Board at the University of Illinois at Chicago waived the need for approval of this secondary data analysis. The study was conducted in accordance with Health Insurance Portability and Accountability Act regulations and adhered to the tenets of the Declaration of Helsinki.
Participant Randomization to Hormone Therapy and Adherence
Randomized treatment assignment was performed in the WHI hormone trial. In the WHI, the women who had previously undergone hysterectomy were randomized to receive either conjugated equine estrogens (0.625 mg/day) or placebo; women with a uterus were randomized to receive oral conjugated equine estrogens and medroxyprogesterone acetate (0.625 mg/day + 2.5 mg/day) or placebo. As reported previously, there were no differences within each randomized trial with respect to patient age, age at menarche or menopause, education, race, annual income, smoking, alcohol consumption, history of hormone use, or the incidence of diabetes mellitus, stroke, myocardial infarction, peripheral artery disease, glaucoma, and cataracts in the WHI hormone trial. For the WHISE study, women aged 65 years and older were recruited from the WHI hormone trial. Participants in the WHISE study were recruited an average of 5.1 (median, 5.0; range, 1–10) years after randomization to the WHI hormone trial.
In the WHI hormone trial, nonadherence to treatment was defined by the parent trial as any of the following: discontinuation of study medications, crossover to the placebo or other hormone group, or <80% adherence based on pill counts from a 6-month supply at any time during follow-up. In the estrogen-alone trial, 53.8% had discontinued study medications by the end of the study, and the rates were equal in the treatment and placebo groups. In the estrogen-plus-progestin trial, 42% of the active estrogen-plus-progestin group and 38% of the placebo group had discontinued treatment by the end of the study. Accordingly, the WHISE study followed the definition of nonadherence for consistency.
Eye Health and General Health Assessment
At the WHISE clinics, participants completed a questionnaire on ocular conditions, including cataracts, glaucoma, early and late AMD, retinal detachment, trauma, previous treatment or ocular surgery, and other eye conditions. During each visit to the WHI or WHISE clinics, participants completed a questionnaire assessing medical history, medical conditions, and lifestyle factors.
Ophthalmic Assessment
Eye examinations were performed at the time of WHISE study recruitment. The examination included visual acuity testing with refraction, anterior segment examination, bilateral standard stereoscopic fundus photography, and IOP measurements. After pupillary dilation to at least 6 mm, the photographer took 30-degree or 35-degree stereoscopic fundus photographs. Fundus photography followed a specified protocol that was adapted for the study by photography consultants at the University of Wisconsin. A single IOP measurement was performed by a Goldmann applanation tonometer (Haag-Streit, Konig, Switzerland) in each eye if the participant reported no known allergy to anesthetic eye drops or fluorescein. If the IOP reading was >30 mm Hg in either eye, the participant was advised to seek further evaluation by her ophthalmologist. As this was a double-masked trial, examiners and participants did not know the patient’s treatment assignment.
Selection Criteria and Statistical Analysis
The final analysis in the current study included all WHISE participants who had IOP data for both eyes. Demographic and clinical characteristics were compared between participants in the treatment and placebo groups. Continuous variables were compared using t tests, and χ 2 tests were used for categorical variables. Multiple linear regression models were conducted to determine the effect of estrogen alone or estrogen plus progestin on IOP compared to that for placebo treatment. Covariates included age, duration of hormone therapy, race, body mass index (BMI), lens status (pseudophakia yes/no, excluding aphakia), adherence, and history of any of the following: diabetes mellitus, hypertension, smoking (never, past, current), and alcohol use (>12 drinks ever). Data from the right and left eyes were analyzed and reported separately. For the primary outcome, an intention-to-treat analysis was performed, and the model included all women with available IOP data (Model 1). To minimize the potential effect of glaucoma treatment on IOP, we excluded women who reported glaucoma or glaucoma treatment (Model 2). For the secondary outcome, analyses adjusted for adherence were performed for all women (Model 3) and for all women except those with self-reported glaucoma or glaucoma treatment (Model 4). All analyses were conducted using SAS statistical software, version 9.0 (SAS Institute Inc, Cary, North Carolina, USA). A P value of less than .05 was considered statistically significant.
Results
Study Sample
All 4347 women enrolled in the original WHISE study had IOP data; 1668 were enrolled in the estrogen-alone trial and 2679 were enrolled in the estrogen-plus-progestin trial ( Figure ). In the estrogen-alone trial, 808 women (48.4%) received active treatment and 860 women (51.6%) received the placebo. In the estrogen-plus-progestin trial, 1397 women (52.1%) received active treatment and 1282 women (47.9%) received the placebo. Demographic and clinical characteristics of the participants included in the WHISE study are presented in Table 1 . In the estrogen-alone trial, the demographic and clinical characteristics of the treatment vs placebo group were balanced, except that the rate of cigarette smokers was higher in the treatment group. Likewise, in the estrogen-plus-progestin trial, the demographic and clinical characteristics of the treatment vs placebo group were balanced, except that the duration of hormone therapy was higher in the treatment group, whereas the rates of adherence and of lens implants were lower in the treatment group.
| Variables | Estrogen-Alone (n = 1668) | Estrogen-Plus-Progestin (n = 2679) | ||||
|---|---|---|---|---|---|---|
| Estrogen (n = 808) | Placebo (n = 860) | P Value | Estrogen + Progestin (n = 1397) | Placebo (n = 1282) | P Value | |
| Age at eye exam (y; mean ± SD) | 72.0 ± 5 | 72.2 ± 5 | .23 | 71.6 ± 5 | 71.7 ± 5 | .46 |
| Duration of hormone use (y; mean ± SD) | 5.0 ± 1 | 5.1 ± 1 | .34 | 5.1 ± 1 | 5.0 ± 1 | .009 |
| Race (%) | ||||||
| White | 84.8% | 83.5% | .06 | 90.1% | 91.9% | .67 |
| African-American | 10.3% | 12.1% | 5.6% | 4.4% | ||
| Hispanic | 3.5% | 2.1% | 2.7% | 2.3% | ||
| Diabetes mellitus, a n (%) | 108 (13.4) | 129 (15.0) | .34 | 133 (9.5) | 113 (8.8) | .53 |
| Hypertension, b n (%) | 313 (39.4) | 334 (39.2) | .94 | 460 (33.0) | 420 (33.1) | .97 |
| Alcohol consumption, c n (%) | 697 (86.6) | 736 (86.1) | .77 | 1248 (89.7) | 1119 (88.1) | .20 |
| Cigarette smoking, d n (%) | ||||||
| Never smoked | 479 (60.0) | 454 (53.5) | .03 | 741 (53.6) | 651 (51.6) | .53 |
| Past smoker | 270 (33.8) | 330 (38.9) | 542 (39.2) | 522 (41.4) | ||
| Current smoker | 50 (6.3) | 65 (7.7) | 99 (7.16) | 89 (7.05) | ||
| BMI (kg/m 2 ; mean ± SD) | 29.6 ± 5.9 | 29.7 ± 5.7 | .71 | 28.5 ± 5.6 | 28.6 ± 6.0 | .58 |
| Self-reported glaucoma, e n (%) | 71 (8.8) | 65 (7.6) | .36 | 98 (7.0) | 94 (7.3) | .75 |
| Adherence to intervention, f n (%) | 298 (36.9) | 352 (40.9) | .09 | 645 (46.2) | 736 (57.4) | <.001 |
| IOP (mean ± SD, in mm Hg) | ||||||
| Right eye | 15.4 ± 3.2 | 15.8 ± 3.3 | .009 | 15.6 ± 3.0 | 15.7 ± 3.1 | .34 |
| Left eye | 15.3 ± 3.1 | 15.9 ± 3.2 | <.001 | 15.7 ± 3.0 | 15.7 ± 3.0 | .54 |
| Pseudophakia, g n (%) | ||||||
| Right eye | 150 (18.8%) | 147 (17.3%) | .45 | 190 (13.9%) | 210 (16.7%) | .05 |
| Left eye | 143 (17.8%) | 136 (16.0%) | .33 | 187 (13.7%) | 209 (16.6%) | .04 |
a The presence of diabetes mellitus was self-reported from the Women’s Health Initiative (WHI) questionnaire and/or the Women’s Health Initiative Sight Exam (WHISE) questionnaire.
b Hypertension was self-reported from the WHI questionnaire.
c Alcohol consumption, determined from the WHI questionnaire, was evaluated using a yes or no response to the following question: “have drunk 12 alcoholic beverages ever.”
d Smoking status was determined from the WHI categorization.
e Self-reported glaucoma or glaucoma treatment was determined from the WHI baseline examination or the WHISE visits.
f Nonadherence was defined as any of the following: discontinued use of study medications, converted to the placebo group or treatment with another, or <80% compliance based on pill counts at any time during follow-up.
Effects of Hormone Therapy on Intraocular Pressure
IOP was measured approximately 5 years after randomization to treatment. In the estrogen-alone trial, for right eyes, the IOP mean ± standard deviation (SD) was 15.4 ± 3.2 mm Hg in the active treatment group and 15.8 ± 3.3 mm Hg in the placebo group. For left eyes, the mean IOP ± SD was 15.3 ± 3.1 mm Hg in the active treatment group and 15.9 ± 3.2 mm Hg in the placebo group ( Table 1 ). In the estrogen-plus-progestin trial, the mean IOP ± SD of the right eye was 15.6 ± 3 mm Hg in the treatment group and 15.7 ± 3.1 mm Hg in the placebo group; the mean IOP ± SD of the left eye was 15.7 ± 3.0 mm Hg in the treatment group and 15.7 ± 3.0 in the placebo group ( Table 1 ).
In Table 2 , the final adjusted analysis included women with available covariates. In the primary models (1 and 3), the final analysis included 4105 women for the right eyes and 4098 women for the left eyes. The secondary models (2 and 4) excluded 328 women who reported glaucoma or history of glaucoma treatment at the WHI baseline examination and/or the WHISE examination. The 328 women who were excluded consisted of 71 women in the estrogen-alone arm and 65 in the placebo arm of the estrogen-alone trial and 98 women in the estrogen-plus-progestin arm and 94 in the placebo arm of the estrogen-plus-progestin trial. In the secondary models (Models 2 and 4), the final analysis included 3798 women for the right eyes and 3,795 women for the left eyes. After adjusting for covariates, the intention-to-treat analysis (Model 1) showed that estrogen-alone treatment was associated with a 0.5 mm Hg lower IOP in the right eye (95% confidence interval [CI]: −0.8, −0.1, P = .005) and a 0.6 mm Hg lower IOP in the left eye (95% CI: −0.9, −0.3, P < .001) when compared to the IOP in the placebo group ( Table 2 ). In the estrogen-plus-progestin trial, there was no significant difference in IOP between the active treatment and placebo groups ( P = .30 in the right eye and P = .43 in the left eye, Table 2 ). Similar findings were observed in Model 2, which excluded 328 women with either self-reported glaucoma or glaucoma treatment at the WHI baseline examination and/or the WHISE examinations. The IOP was significantly lower in the estrogen-alone treatment group compared to that in the placebo group for both the right and left eyes, and there was no significant effect of estrogen-plus-progestin treatment on IOP ( Table 2 ). Compared to the IOP in the placebo group, estrogen-alone treatment was associated with a 0.5 mm Hg lower IOP in the right eye (95% CI: −0.8, −0.2, P = .005) and a 0.6 mm Hg lower IOP in the left eye (95% CI: −0.9, −0.3, P < .001) ( Table 2 ). In the estrogen-plus-progestin trial, there was no significant difference in IOP between the active treatment and placebo groups ( P = .54 in the right eye and P = .62 in the left eye, Table 2 ). Similar findings were observed in the adherence-adjusted analyses (Models 3 and 4, Table 2 ).
| Trials | Estrogen-Alone | Estrogen-Plus-Progestin | ||
|---|---|---|---|---|
| Right Eye | Left Eye | Right Eye | Left Eye | |
| Primary outcome: Intention-to-treat analysis | ||||
| Model 1: All women | ||||
| All | n = 1584 | n = 1582 | n = 2521 | n = 2516 |
| β | −0.46 | −0.60 | −0.13 | −0.09 |
| (95% CI) | (−0.78,−0.14) | (−0.91, −0.29) | (−0.37, 0.11) | (−0.32, 0.14) |
| P value a | .005 | <.001 | .30 | .43 |
| Model 2: Excluded women with self-reported glaucoma or glaucoma treatment b | ||||
| All | n = 1454 | n = 1453 | n = 2344 | n = 2342 |
| β | −0.47 | −0.57 | −0.08 | −0.06 |
| (95% CI) | (−0.80,−0.15) | (−0.89, −0.25) | (−0.32,0.17) | (−0.30,0.18) |
| P value a | .005 | <.001 | .54 | .62 |
| Secondary outcome: Adherence-adjusted analysis | ||||
| Model 3: All women | ||||
| All | n = 1584 | n = 1582 | n = 2521 | n = 2516 |
| β | −0.45 | −0.60 | −0.14 | −0.11 |
| (95% CI) | (−0.77, −0.13) | (−0.91, −0.28) | (−0.38, 0.10) | (−0.35, 0.13) |
| P value a | .006 | <.001 | .26 | .36 |
| Model 4: Excluded women with self-reported glaucoma or glaucoma treatment b | ||||
| All | n = 1454 | n = 1453 | n = 2344 | n = 2342 |
| β | −0.46 | −0.57 | −0.08 | −0.07 |
| (95% CI) | (−0.79, −0.13) | (−0.89, −0.24) | (−0.33, 0.16) | (−0.31, 0.17) |
| P value a | .006 | <.001 | .50 | .57 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


