malignancy. Imaging and biopsy for culture/pathologic diagnosis should be performed quickly and aggressive medical and surgical interventions instituted immediately should fungal infection be found.
TABLE 33.1 Chandler Classification of Orbital Complications | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||
recurrent disease should undergo immunologic workup as well as imaging to look for anatomic issues that may predispose to orbital infections (Fig. 33.2).
 FIGURE 33.1 A: Edema and erythema of the left eyelid in a young child with a left SPOA. B: Axial CT image of left SPOA (arrow). |
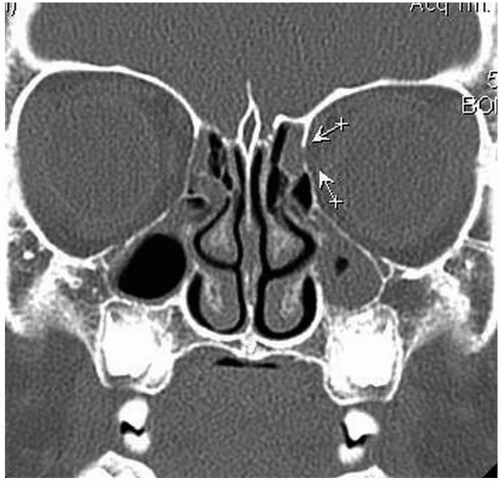 FIGURE 33.2 Coronal CT scan of the sinuses, taken during a disease-free period, of a child who has had three episodes of orbital cellulitis. Note the defect in the left lamina papyracea (arrows) adjacent to an opacified ethmoid cell. |
attempted although such assessment may be difficult in a sick young child. Pupil reactivity should be normal, and the presence of an afferent papillary defect is an ominous sign. The presence and severity of proptosis and/or restriction of gaze suggests postseptal orbital involvement and possible abscess formation. Eyelid fullness, position, and elevation should be assessed, as advanced orbital infections can be accompanied by infection in the lid spaces.
 FIGURE 33.3 A toddler with right ethmoid sinusitis and SPOA. Note upper>lower eyelid edema and erythema. |
TABLE 33.2 Criteria for Medical Versus Surgical Management of Subperiosteal Orbital Abscesses | |||
|---|---|---|---|
|



