The evolution of the facelift during the twentieth century was dependent on technologic breakthroughs and the understanding of the anatomy responsible for the vagaries of aging. With better lighting and the development of low-reacting suture materials that self-absorbed over weeks and months, surgeons were able to see, manipulate, and secure tissue planes that were previously impossible to work with. During the early 1900s, simple skin excision with minimal if any undermining was the standard.1 With fiberoptic lighting, dissection could be extended farther and farther under the skin with improved results. As late as the 1960s and 1970s, the need to do little more than lift the skin remained controversial. With Mitz and Peyronie’s2 landmark anatomic work on the subcutaneous musculoaponeurotic system (SMAS), the innovators were stimulated to plicate, imbricate, excise, and manipulate this layer in a variety of ways. Depending on the approach used by a specific surgeon, varying degrees of success and longevity could be added to the standard skin-flap facelift. It was not until Hamra3 fully mobilized the SMAS layer in continuity with the obicularis oculi muscle to release the zygomatic ligament that the deep-plane facelift came into practice. The old controversy of the need to even operate on the subcutaneous layers now had added an extra caveat: Does the deep-plane lift improve the mid-face laxity and the overall results of a SMAS-manipulated facelift, to justify the increased risk and morbidity to the patient?
Background
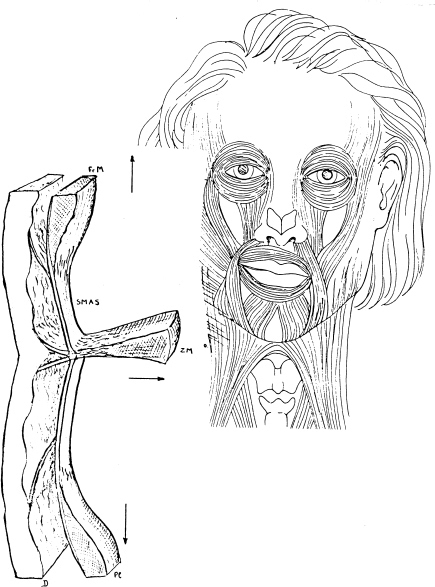
Aufricht4 defined the SMAS layer in his article reviewing 15 years of SMAS surgery as “the area overlying the parotid and underlying the skin of the face and cheek. This sheet, present in the embryo, is made of fibrous tissue and of some muscular fibers; superiorly, it is related to the obicularis and frontal muscles and inferiorly by the platysma. Lying between the muscles of facial expression and the skin, it arches over the zygoma and stretches from the tragus to the nasolabial fold, fanning into labial musculature”; (Fig. 25–1). Aufricht4 was among the first to advocate plication of this fibrous layer in an effort to enhance the postoperative result and achieve a longer lasting result. Skoog5 also popularized the manipulation of this layer to improve the results.
IMBRICATION
Webster et al.6 performed a series of operations in 1982 in which they attempted to show that imbrication, the undermining and advancement of the SMAS, failed to increase the amount of posterior displacement of aesthetically important landmarks as compared with simple plication of this layer. Despite these results and an ongoing debate in the literature concerning the efficacy of SMAS surgery, the standard approach to the SMAS is extensive freeing of the skin in the cheek area to the cheek-lip fold. In the neck, the skin is undermined across the midline in most patients. When imbricating, the SMAS is incised horizontally 1 cm below the zygomatic arch. The vertical limb runs inferiorly in front of the ear to connect with the platysma along the anterior border of the sternocleidomastoid muscle. The dissection of this SMAS flap extends to the anterior border of the parotid gland, avoiding any injury to the facial nerves. As the SMAS runs in continuity with the playsma, the extent of the subplatysmal dissection can vary from 1 to 2 cm, to meet in the midline, negating the need for a submental incision.7 This SMAS flap is then advanced posteriorly and superiorly. The excess is excised above the zygomatic arch and in front of the ear with subsequent reapproximation of the cut edges. The posterior flap is sutured to the sternocleidomastoid fascia. Present-day PDS sutures permit ample time for fibrosis and healing before being absorbed 6 months later.
PLICATION
Plication of the SMAS layer involves the same amount of skin undermining as for imbrication, but this layer is not incised. Approximately 3 cm below the zygomatic arch, the SMAS is grasped with a pair of forceps and pulled posteriorly and superiorly while the effect on the skin flap, ptotic jowl fat, and labial commissure is observed. The goal is to advance and elevate the SMAS layer and the contiguous structures as much as possible. Once this point is found, double-looped sutures of 3/0 PDS are placed through it to fix and tighten this pseudofascial layer.
The deep-plane facelift described by Hamra3 was an extension of the sub-SMAS facelift, with the dissection extending beyond the anterior border of the parotid, superiorly over the malar eminence, and anteriorly into the nasolabial fold. Inferi-orly, itstops at the jawline. The skin is undermined only 2 to 3 cm before creating a composite musculocutaneous flap that stays above the zygomaticus muscles to release the zygomatic ligaments. When the SMAS is released, the skin, subcutaneous fat, and fascial layers are all elevated and advanced superoposteriorly. The dermis of the flap is secured with absorbable sutures to the temporal fascia.
Discussion
The search for perfection and the multitude of articles published annually attest to the fact that the ultimate universal facelift has yet to be discovered. I might add that it will never be—the aesthetics, surgical ability, patient’s anatomy, and desires offer too great a variability to be defined by one operation. What is enlightening is the multitude of facelift procedures being used to correct the vagaries of the aging process. During the early 1980s, I formulated a classification of the neck.9
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


